
Cellular constituents that may be present in urine include leukocytes, erythrocytes, epithelial cells and sperm. Please also refer to the compilation table of cells that may be seen in the urine and the urinalysis atlas. Evaluation of cellular constituents requires concentration of urine in some way, most commonly done by centrifugation, but gravity sedimentation of urine within a microtiter plate can also be done (and visualized by an inverted microscope, which is likely only available in select laboratories) (Chase et al 2017). The volume of centrifuged urine will also likely influence the numbers of cellular constituents in the smear. It can be difficult to standardize this volume, when veterinary laboratories frequently receive a range of volumes to examine (<0.5 to >100 mL). In our laboratory, we standardize the urine volume to 5 ml whenever possible.
White blood cells
White blood cells (WBC) are reported semi-quantitatively as the number seen per high power field (HPF) using the high dry objective (40x):
Interpretation
Less than 5 WBC/HPF is commonly accepted as normal (however, it is unclear on where this number was derived from and in a clean urine [e.g. minimal hematuria, cystocentesis collection, <5 WBC/HPF could very well be abnormal). Greater numbers (pyuria) generally indicate the presence of an inflammatory process somewhere along the course of the urinary tract (or urogenital tract in voided specimens). Pyuria often is caused by urinary tract infection, and many times bacteria can be seen on sediment preps. Depending on clinical signs, pyuria may be an indication for culture of urine even if no bacteria are seen. Non-septic causes of inflammation, such as uroliths and tumors, also must be considered.
Identification
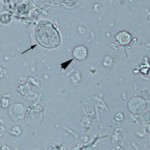
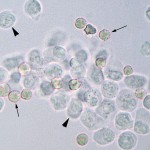
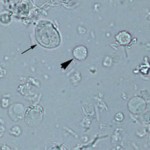
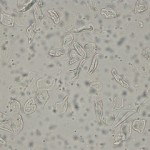
In regular unstained urine sediments, WBC are small cells, usually 1.5 – 2 x larger than a RBC (see image below), are regularly round, colorless and have a slightly grainy appearance. Like erythrocytes, WBC may lyse in very dilute or highly alkaline urine. The type of WBC (neutrophil, lymphocyte, monocyte etc) cannot be determined from a regular urine wet preparation, but they are usually neutrophils. A cytologic examination would be required to determine which WBC types are present in urine, however this is rarely indicated for this purpose.
WBC must be distinguished from RBCs and small epithelial cells.
- WBC vs RBC
The grainy nature of WBC helps to distinguish WBC from RBC which are smoother. WBC are also colorless whereas RBC are slightly red-tinged from hemoglobin. Identification of the segmented nuclear shape of a neutrophil is helpful, but this feature is often inapparent, particularly if the specimen is not fresh (the nucleus swells and rounds up with storage).
- WBC vs small epithelial cells
This distinction is far more difficult and may rely on cytologic examination of the urine sediment. WBC are generally smaller than epithelial cells and are more round (note that WBC can swell with storage and appear larger than normal). Epithelial cells have more angular borders or polygonal shapes and round to oval nuclei.
Red blood cells
Red blood cells (RBC) are reported semi-quantitatively as number seen per high power field (HPF):
none seen; <5, 5-20, 20-100, or >100/HPF.
Interpretation
Up to 5 RBC/HPF generally are considered acceptable for “normal” urine, although this depends on the mode of collection (little blood is expected with voided samples, unless there has been contamination from the genital tract, e.g. dogs in estrus).
Increased red blood cells in urine is termed hematuria, which can be due to hemorrhage (e.g. idiopathic renal hematuria in young large breed dogs [Di Dinato P et al 2019], hemorrhagic cystitis in horses [Smith et al 2018]), or hemorrhage due to inflammation, necrosis, trauma, or neoplasia somewhere along the urinary tract (or urogenital tract in voided specimens). The hemorrhage can originate from anywhere in the urinary tract, as well as the genital tract (in voided or catheterized specimens).
The method of collection should be considered when interpreting hematuria in order to aid in localization, and also because catheterization, cystocentesis, and manual compression can cause iatrogenic hemorrhage (with cystocentesis, it is usually a microscopic hematuria with as many as >100/HPF in a grossly yellow urine that is not accompanied by proteinuria).
Red blood cells with abnormal shapes (dysmorphic) in urine (e.g. RBCs with blebs or protrusions) are thought to reflect glomerular injury, such as glomerulonephritis. They are seen in higher percentages of patients with glomerular disease but can also be seen with lower urinary tract disease, e.g. urothelial cancer (Crop et al 2010, Koo et al 2016).
Identification
The appearance of red blood cells in urine depends largely on the concentration of the specimen and the length of time the red blood cells have been exposed.
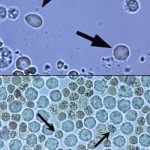
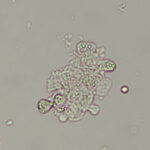
In fresh urine, RBCs are round smooth cells and are slightly red-tinged (from hemoglobin). In fresh samples with specific gravity of 1.010-1.020, RBC may retain their normal disc shape, particularly in dogs. In more concentrated urine (>1.025), red blood cells lose their smooth texture, tend to shrink and appear as small, crenated cells (see image to the right). In more dilute samples, they tend to swell. At urine specific gravity <1.008 and/or highly alkaline pH, red blood cell lysis can occur. Lysed red blood cells appear as very faint “ghosts”, globules of hemoglobin (see urine cell album) or may be virtually invisible. However, a heme reaction (reaction for “blood”), often 4+, on the dipstick will be evident. Red blood cell lysis, regardless of cause, will be indistinguishable from hemoglobinuria and myoglobinuria, so a hemogram and biochemical panel should be evaluated concurrently for a hemolytic anemia with intravascular hemolysis and severe muscle injury, respectively.
Epithelial cells
Different types of epithelial cells can be observed in urine. Some of these are readily identifiable, however it is difficult to distinguish small transitional epithelial cells from WBCs and renal tubular epithelial cells from transitional epithelial cells. Thus, all non-squamous cells in urine are considered to be of transitional origin. When unsure about the origin of the cells in urine, we can stain a urine sediment with a modified Wright’s stain (or rapid stain such as Diff-Quik®, Quick stains, Hemacolor® etc) and perform a cytologic examination on the urine sediment.
Epithelial cells are subjectively semi-quantified in urine (usually under low power using the 10x objective) as: none seen, few, moderate, many
Neoplastic cells of renal, urinary or reproductive origin can exfoliate in the urine and a urinalysis is definitely indicated if a tumor in one of these sites is suspected in the animal. Examination of a regular urine sediment preparation can be the first clue to identification of neoplastic cells, however the diagnosis of neoplasia is based on cytologic criteria of malignancy in the cells, which are not easy to discern in these wet preparations. Thus, we recommend that a cytologic analysis of the urine (using a standard hematologic stain, such as a modified Wright’s stain) is performed if neoplasia is suspected.
Transitional epithelial cells
The urinary tract from the pelvis down the ureters to the bladder and the proximal urethra is lined by transitional epithelial cells. These cells vary in size and shape depending on the location from which they originate, e.g. those from the renal pelvis are more caudate whereas those from the bladder are more round to polygonal and vary in size (Batamuzi and Christensen 1995). These cells naturally slough into the urine in quite low numbers, so none to a few transitional epithelial cells are seen in the urine from healthy animals. Note that this depends on the method of urine collection, since these cells may be sloughed (traumatically) in excess numbers and even in sheets when the bladder is catheterized.
Transitional epithelial cells must be distinguished from WBC, because they both have the same granular appearance. In general, transitional epithelial cells are larger and have more irregular borders than WBC (which are uniformly more round; see image on right). However, it can be difficult to differentiate small epithelial cells from WBC in a wet mount of urine. If in doubt, perform a cytologic smear of the urine sediment.
Squamous epithelial cells
These can be keratinized or non-keratinized.
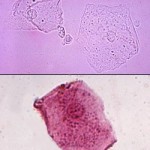
Non-keratinized squamous epithelial cells originate from the distal urethra, prepuce and/or vagina and extend from the bladder trigone (Batamuzi and Christensen 1995). They are larger than transitional cells and have small central nuclei. They can be round or have one or more flat border. Keratinized squamous epithelial cells are from the the skin or vulva and are large cells with angular borders. They may or may not have nuclei (see image to the right). Nuclei are more visible in cells when the urine is stained with Sedi-stain (see lower panel of second image on the right). If in doubt about the origin of the cells, a Wright’s stain (routine hematologic stain) can be performed on a urine sediment and demonstrates the central nuclei and angular borders of squamous epithelial cells.
Squamous cells are frequently seen as contaminants in voided urine samples and can also contaminate samples collected by catheterization. Urine collected by cystocentesis should not contain any squamous epithelial cells.
Note that although these cells are considered contaminants, large numbers may represent abnormal genitourinary conditions, specifically squamous metaplasia of the prostate in the dog. This occurs secondary to excess estrogen, usually secreted by testicular tumors (particularly Sertoli cell tumors, but this has also been reported with interstitial cell tumors).
Renal tubular epithelial cells
Renal tubular epithelial cells are rarely seen in the urine and, as mentioned above, are very difficult to distinguish from transitional epithelial cells. If large numbers of smaller epithelial cells of uniform appearance (size and shape) are observed in the urine, a renal origin for these cells is suspected. Transitional epithelial cells tend to be more variable in size and rounder in shape (to some extent), although they may have caudate (tailed) shapes (caudate cells are thought to line the renal pelvis or calyces). Squarer or rectangular cells, the presence of a squared off or blunt end (supporting a columnar shape) are features of renal tubular cells. Columnar cells are more likely to come from the collecting ducts versus the upper renal tubules. The presence of moderate or many renal tubular epithelial cells in a urinalysis supports renal tubular injury.
Neoplasia
Neoplastic cells, typically those of transitional epithelial origin (transitional cell carcinoma or TCC) may slough into the urine. The presence of these cells can be diagnostic of urinary neoplasia, however they are not always seen in the urine in affected animals. Thus, the lack of these cells in a urinalysis does not rule out neoplasia.
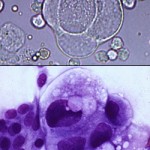
TCC are more common in dogs and frequently originate in the trigone of the urinary bladder. The urethra of male and female dogs (prostatic urethra for males) is also a common site, with prostatic urethral TCC often invading the prostate, mimicking primary prostatic carcinomas. Diagnosis of neoplasia depends upon the identification of cytologic criteria of malignancy in the epithelial cells, e.g. marked variation in nuclear and cell size (anisokaryosis and anisocytosis, respectively), multiple nucleoli of variable size within one nucleus, multi-nucleation with intracellular anisokaryosis, macronucleoli. These features are only reliably discernable in cytologic smears (stained with a hematologic stain such a rapid stain or modified Wright’s stain) and are difficult to impossible to identify with confidence in an unstained preparation of urine (see image above right). Thus, a urine cytology should be performed on animals with suspected tumors.

TCC usually invade the bladder wall and cause hemorrhage. They may also become secondarily inflamed from necrosis or a superimposed bacterial infection. Thus, hematuria and, to a lesser extent, pyuria, can be features of a urinalysis in animals with TCC.
Rarely, other tumors originating in the bladder or kidney (e.g. lymphoma, renal carcinoma) can exfoliate into the urine. Pictured right are images from an unstained and Wright’s stained urine sediment from a cat with renal lymphoma. The neoplastic lymphoblasts had exfoliated into the urine and provided the diagnosis in this case.
Sperm

Sperm in urine generally are of significance only as a testament to the intact maleness of the donor. They may be seen in urine from males collected by voiding, catheterization, or cystocentesis. Rarely, they may be observed in voided urine from a recently-bred female. The presence of sperm is reported as part of the complete sediment examination, the goal of which is to report all microscopic findings.
Related links
- Cell quick guide: A compilation table of cells that may be seen in the urine
- Urinalysis atlas.
- References:
- Haber MH et al. Color atlas of the urinary sediment. An illustrated field guide based on proficiency testing. College of American Pathologists, Associated Press, 2010.
- Osborne CA and Stevens JB: Urinalysis: A clinical guide to compassionate patient care, 1999.
- Ringsrud KM and Linné JJ. Urinalysis and body fluids. A color text and atlas. Mosby, 1995.