
Total solids

Total solids is used as an estimate for total protein (which are the constituents of plasma that have the most effect on the refractive index). Total solids are measured by refractometer and actually measures refractive index. This is used as a quick guide as to potential mechanisms for anemia (e.g. a low total protein would support blood loss) or the presence of other disorders (e.g. a very high total protein, with accompanying rouleaux formation in erythrocytes indicates hyperglobulinemia, which may be due to inflammation or B or plasma cell neoplasia). This quick assessment is not always provided on hemogram results. Remember that this assessment is done on plasma (which contains fibrinogen), so values are usually higher than that seen on chemistry panels run on serum (which lacks fibrinogen). More accurate values for total protein are obtained from our chemistry analyzer and chemistry panels.

The following technique applies to manual (optical) refractometers. Digital refractometers are now available as well. To perform total solid assessment using a manual refractometer, a microhematocrit tube is filled with EDTA-anticoagulated blood using capillary action. The tube is then sealed, placed in a microhematocrit centrifuge, centrifuged for 3 minutes (or longer) and then removed from the centrifuge. The tube should consist of packed red blood cells (at this stage, a packed cell volume or PCV can be measured), the buffy coat (platelets and WBC) and overlying plasma (the color/nature of the supernatant plasma can be visually assessed – see below) (see image to right). Ideally plastic microhematocrit tubes (which cannot be broken, e.g. SAFE-CAP® plain capillary tubes) and a plasma-expeller (e.g. SAFEPETTE® dispenser), which transfers the plasma to the refractometer should be used. However, these are not always available and glass microhematocrit tubes can be used. If a glass tube is used, the tube can be “scored” above the buffy coat, using a diamond pen or the side of a microscope slide, i.e. the pen or side of the slide is used to create a scored line in the tube (see image to right). The tube should then be able to be cleanly broken at the scored line (if the line is scored well enough – sometimes the tubes break during scoring). The unbroken end of the tube containing plasma is then placed at the interface of the refractometer lid (closed as shown in the top image) and refractometer transferring the plasma to the window by capillary action or gently tapping the end of the tube to the interface (try to avoid tapping the tube directly onto the glass window as this will damage the glass). The refractometer plate is then closed on top of the plasma and the interface between the light and dark regions is identified through the visualization window. This should be a sharp line. The corresponding number at the interface is equivalent to the value for total solids. Note, that this method (using glass tube and scoring the tube) is not recommended due to safety concerns. Also, NEVER blow on the end of the tube to remove the plasma (major major biosafety hazard, let alone getting cut on the glass). For more on measurement of total protein by refractometer, refer to a review by George 2001.
Digital refractometers provide similar values to optical or manual refractometers, although they will provide a reading below the limit of detection of manual refractometers (<0.25 g/dL). They similarly over-estimate total protein concentrations compared to a chemistry analyzer, however they are less affected by hemolyzed samples (both refractometers and chemistry analyzers will measure the free hemoglobin as protein).
-
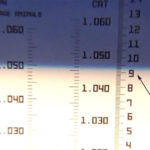
The refractometer line Increased values:
- False change: An increase in non-protein solids, including electrolytes (particularly sodium and chloride) and other chemical constituents of plasma (lipids, glucose, urea nitrogen, creatinine) will increase the refractive index. The worse offenders are glucose (>300 mg/dL) (Carigan et al 2023) and lipid, particularly chylomicrons (because they are so large) but also high concentrations of very low density lipoproteins. Indeed, results are usually falsely increased by lipemia (increased chylomicrons or VLDL or both), hence the total protein by refractometer result on our hemograms is usually cancelled when lipemia is present. Hemolysis makes the refractive line more difficult to read on manual refractometers, but does not appear to affect digital refractometers to the same extent (Carigan et al 2023). We still, however, may cancel the total protein result on our hemograms if the sample is severely hemolyzed, even with using digital refractometers. Icterus does not affect the measurement. When bilirubin was spiked into serum from 2 Greyhounds, there was no effect on total solid estimation using three different refractometers from Leica with concentrations as high as 41.5 mg/dL. Results from the three refractometers varied by 0.1-0.4 g/dL without any association to bilirubin concentrations (Gupta and Stockham 2014). This shows the inherent variability of refractometers. Internal studies at Cornell University on canine and equine plasma has shown that digital (Misco Palme Abbe) and manual (Leica) refractometers have a precision of 0.5-2.6% (acceptable) with an absolute difference of 0-0.4 g/dL between repeat measurements, similar to the study by Gupta and Stockham and that by Carigan et al 2023.
- Increased protein: High total solids that is not due to changes in total solids is usually interpreted as an increase in total protein concentraiton, which can consist of albumin and globulins or both. However, very high total protein concentrations (>9.0 g/dL) are usually due to an increase in globulins. Since the test is run on plasma, the globulins will include fibrinogen.
- Decreased values: Any cause of protein loss (e.g. blood loss, protein-losing enteropathy or nephropathy), protein catabolism, or decreased intake of protein (e.g. malnutrition). Immunodeficiencies, such as that due to failure of passive transfer of immunity, can also result in a low protein concentration. Protein concentration can also be low in young growing animals as a physiologic response.
Plasma appearance

The gross appearance of the plasma in the microhematocrit or centrifuge tube can provide useful information, quickly and reliably.
- Yellow discoloration of the plasma, though normal (within limits) in horses and cattle (due to carotenoids), is evidence of hyperbilirubinemia (icterus) in dogs and cats. This is termed icterus and is graded mild, moderate or marked (subjectively). The chemistry analyzer gives a more numerical assessment of this color change with the icteric index.
- Red color in the plasma indicates the presence of free hemoglobin. This is most often due to artifactual disruption of RBC during sample collection and/or handling (in vitro hemolysis), but can also been seen in cases of intravascular hemolytic disease. Like the other features of plasma, we subjectively grade hemolysis as mild, moderate and marked. Our chemistry analyzer provides a numerical assessment of the amount of hemoglobin in the sample as a hemolytic index.
- Whitish opacity of the plasma indicates hyperlipidemia and is associated with increased concentrations of triglycerides (triglycerides dominate) usually due to high chylomicrons or very low density lipoproteins. Though most often associated with the normal post-prandial state in dogs and cats, pathologic hyperlipemia can be seen in ponies and certain breeds dogs (e.g. Schnauzers), and in cases of acute pancreatitis, hyperadrenocorticism, nephrotic syndrome, or hypothyroidism. This is subjectively assessed on our hemograms as mild, moderate or marked and falsely increases total protein by refractometer measurements (see above) as well as chemistry test results. Our chemistry analyzer gives an approximate measurement of the amount of turbidity in the sample, called the lipemic index.