
Blood for hematologic testing must be collected into an anticoagulant, preferably EDTA (purple top tube). Blood smears should be made at the time of collection to minimize storage-associated changes, which invariably occur. Venipuncture should be minimally traumatic to minimize platelet activation and should be done using a minimum of a 23G needle (21-22G is ideal for small animals and 18-20G is ideal for large animals) and 3-5 mL syringe (depending on the desired volume). Vacutainers can be used for sample collection, as can short butterfly catheters. For very small or pediatric patients, samples can be placed into microtainer tubes. Regardless of the tube used for sample collection, the blood must be adequately mixed with the anticoagulant during and after collection to prevent clotting. This is done by gentle inversion of the tube (tubes should never be shaken).
View other sample collection pages specific for hemostasis, chemistry, urinalysis and cytology.
Sample collection and handling guidelines

All samples should be kept cool (at refrigerated temperatures, but not frozen) during storage and shipping to minimize changes in cells that can occur with storage. The sample should be wrapped in paper towels to prevent direct contact of the tube with ice, which will result in freezing and lysis of red and white blood cells within the tube. Also, blood smears should be made from freshly collected blood and submitted along with the tubes to help facilitate blood smear examination and ensure provision of the most accurate results. The blood in the tube should be kept cold, however slides should be stored and shipped at room temperature. Both tubes and slides should be placed in break-proof containers for shipping.
The following anticoagulants can be used for hematologic testing, however EDTA (purple top) is the preferred anticoagulant.
- EDTA: Cell preservation is optimal in this anticoagulant, which chelates calcium, preventing clotting. High concentrations of EDTA are hypertonic in comparison to red blood cells, so if only a small amount of blood is collected (e.g. 0.5 mL) and placed into a standard 5 mL EDTA tube, the red blood cells will shrink (see collection artifacts below). Rarely, exposure of blood to EDTA can result in the binding of antibodies in the animal’s plasma to platelets or red blood cells. The consequence of antibody binding to platelets is that platelets aggregate (clump) resulting in a falsely decreased platelet count. With antibody binding to red blood cells, red blood cells aggregate, mimicking agglutination which is a key feature in red blood cells that is usually diagnostic for immune-mediated hemolytic anemia. In this scenario, it is an artifact but can lead to an erroneous diagnosis of immune-mediated disease (Schaefer et al., 2009). Binding of EDTA-dependent antibodies to platelets and red blood cells can be overcome by collecting blood into citrate anticoagulant, however routine collection of blood into citrate is not recommended for reasons indicated below.
- Citrate: Citrate anticoagulant also chelates calcium, but is a gentler chelator than EDTA. Thus, we can add calcium back to the tube to perform hemostasis testing. The blood is diluted by the citrate anticoagulant (by 10% if the appropriate volume ratio of blood to citrate is maintained, i.e. 1 part citrate to 9 parts blood), therefore all counts will be lower by at least 10% compared to blood collected into EDTA. However, a study on canine platelets has shown that the platelet count is still under-estimated in citrate samples compared to EDTA-anticoagulated samples, even taking into account the 10% dilution effect. In addition, platelets appeared larger and less granulated in citrate anticoagulant, suggesting that they were activated (Stokol et al., 2007).
- Heparin: Heparin is not recommended for hematologic testing. Platelets and leukocytes frequently clump in heparin, causing erroneous counts (absolute counts and a differential leukocyte count). Heparin also introduces a staining artifact (smears look a garish pink-purple) which affects blood smear examination.
Artifacts
Artifacts in blood samples for hematologic testing stem mainly from either sample collection, aging of sample, or poor maintenance of the staining solutions (stain precipitate and water artifact). See also a summary of some of these artifacts.
Collection artifacts
These are associated with problems with sample collection. The most common problems are:
- Difficult venipuncture: Slow or traumatic venipuncture (poking around a lot for the vein, exiting the vein during sample withdrawal) can precipitate platelet clumping and induce small microclots within the sample or even clotting of the sample. Clotting of the sample will decrease all blood counts and invalidate the counts, if severe. Microclots can also be drawn into hematology analyzers and can plug the tubing, causing the machine to malfunction. Difficult venipuncture, particularly through a small gauge needle, can result in shearing of red blood cells (artifactual hemolysis), which affects cell counts and mimics true intravascular hemolysis.
- Low sample volume: Collection of a small blood volume (e.g. 0.5-1 mL) with placement into a standard 5 mL EDTA tube will cause shrinkage of red blood cells, because EDTA is hypertonic. This will cause a false decrease in the mean cell volume (MCV) and false increase in mean cell hemoglobin concentration (MCHC) of red blood cells. Crenation of red blood cells (echinocyte formation) will also be evident on the blood smear. This is a common artifact that we see in hematologic samples. If only a small sample of blood is obtained, a microtainer tube containing EDTA anticoagulant is preferred, but be sure to thoroughly mix the tube (by gentle inversion, several times).
- Inappropriate mixing with anticoagulant: The blood should be thoroughly mixed with anticoagulant during or immediately after sample collection (by several gentle inversions). Collection directly into a vacutainer tube (allowing the vacuum to draw the appropriate amount of blood) is optimal, but difficult to achieve in small or pediatric patients with small veins, that collapse easily. Inadequate mixing will result in sample clotting, which may not be visible to the naked eye (microclots).
- Dilution with fluids: Collection of blood for hematologic testing through an in-dwelling catheter is not optimal, but may be necessary in critically ill patients that are being frequently sampled for monitoring of changes. Ideally, the catheter should be flushed with sterile saline (to remove any contaminating intravenous fluids) and the first 3 mL of blood should be discarded to avoid dilutional effects.
- Rough handling: Shaking of blood tubes, forcing blood through needles, vigorous expulsion into tubes, can cause shearing of red blood cells (hemolysis) and platelet clumping. Samples should be handled with kid gloves.
Storage artifacts
Storage of blood can result in many false changes in hematology results. These changes are minimized but not eliminated by cold storage (refrigerated, shipping on ice packs). Ensure that the slides are maintained at room temperature and are not stored cold or placed in direct contact with ‘”cool packs”, as the slide can freeze or become moist, thus rupturing the cells.
Artifacts of specimen handling and preparation can significantly impair examination of blood cells, but are easily avoided. If a delay in analysis is anticipated (e.g., lab closed or when sending a sample to a reference lab), smears should be made and sent along with the EDTA tube. Air-dried unfixed smears hold up very well unless subjected to flies or moisture.
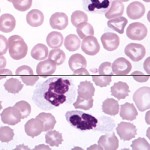
In vitro aging of blood cells in the specimen tube causes changes in the appearance of the cells on stained blood films. Eventually, cells will break down altogether, rendering the specimen useless for analysis. Shown on the right is a smear from a sample which had been in EDTA for 48 hours at room temperature. Extreme crenation of the erythrocytes is evident, which could easily mask or render suspect significant pathologic shape abnormalities. The leukocyte nucleus has undergone pyknosis and karyorrhexis, making certain identification impossible.
Age-related changes that occur are:
- Red blood cells: crenation (echinocyte formation), lysis (this will decrease the RBC count and HCT, leading to a falsely high MCH and MCHC), hemoglobin crystallization. Red blood cells also swell with storage (take up water). This causes a falsely increased mean cell volume (MCV) and decreased mean cell hemoglobin concentration (MCHC). Because the HCT is dependent on the MCV, the HCT may be higher than normal.
- White blood cells: Swellling and smoothing of the nuclear chromatin (mimicking band neutrophil formation), pyknosis and karyhorrhexis of nuclei, cell smudging, and prominence of Döhle bodies (mimicking toxic change). Dohle bodies can start to develop within 4, 8 and 24 hours when EDTA-anticoagulated blood is kept at room temperature, on ice or at 4ºC, respectively (Bau-Gaudreault and Grimes 2019). Pyknotic leukocytes resemble (and can be misinterpreted as) nucleated red blood cells. These changes can decrease a white cell count (lysed cells are not counted) and can affect the accuracy of a differential cell count. Sometimes, the changes are so severe, that an accurate differential cell count cannot be performed.
- Platelets: Clumping, degranulation (the latter makes platelets difficult to see and enumerate). Platelet clumping decreases the platelet count and increases the mean platelet volume (MPV), since a small clump of platelets is seen as a single large platelet. Large platelet clumps are excluded from the count altogether.
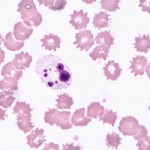
48 hr old blood sample with extreme RBC crenation
Stain artifacts
Diff-Quik®, Hemacolor®, and other commonly used quick stains for hematology and cytology can provide good staining quality if properly used and maintained:
- Keep tightly capped when not in use: This prevents evaporation, minimizes contamination of solutions, and prevents water from the air getting into the fixative.
- Do not “top-off” the solutions: When fluid level drops or staining quality declines, empty, clean, and dry the jars, then refill with fresh solution.
Common stain-related artifacts are water artifact and stain precipitate.
-
Stain precipitate 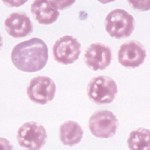
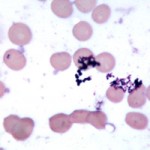
Water artifact Water artifact: When severe, this results in a moth-eaten appearance to the cell. It is a refractile artifact that results from the presence of water in the fixative; it usually occurs when using poorly-maintained quick stains. Refractile means that, as one focuses up and down on the cell, the artifact “flashes”; in one plane of focus, it may appear dark, while in another plane it appears bright. Such artifact, is often mistaken for someform of red blood cell inclusion, such as a parasite (e.g. hemotropic Mycoplasma species).
- Stain precipitate: This usually results from the use of aged staining solutions and/or inadequate rinsing of slides following application of stain. Shown at right is a smear in which large obvious aggregates of stain precipitate are overlying the red cells. Notice how the precipitate is in a different plane of focus than are the cells. Finer precipitate can effectively mimic epicellular parasites or bacteria, and, at the very least, is quite distracting.
Related resources
- Instructional videos on making and staining a blood smear