
Clues as to the underlying presence of liver disease and the nature of the disease (i.e. our four pathologic processes of injury, cholestasis, altered function or blood flow) are derived from all screening clinical pathologic tests – the hemogram, biochemical profile, and urinalysis – as outlined below. Of course, history, signalment, clinical signs and results of other diagnostic testing (ultrasound examination, abdominal radiographs) all help consolidate evidence for liver disease. Results from all this testing then dictate further procedures (e.g. aspiration or biopsy of the liver, peritoneal fluid analysis), which can provide the specific diagnosis.
Hemogram
The hemogram may be absolutely normal in animals with liver disease, but sometimes there are findings that should make us think about underlying liver disease (which should then be confirmed through other diagnostic testing).
- Erythrogram: This can be normal in animals with liver disease, but some animals have a normocytic normochromic anemia due to inflammatory disease (even if the disease process in the liver is not inflammatory in nature).
- RBC indices (MCV, MCHC): As indicated above, these are usually normal in liver disease, however some dogs with portosystemic shunts (acquired or congenital) can have microcytosis (low MCV) which may or may not be accompanied by hypochromic RBCs (low MCHC). The red blood cell distribution width (RDW) can also be increased. The cause of these RBC changes is unknown but has been attributed to a “functional” iron deficiency due to abnormal iron metabolism (body iron stores may be normal). In a surgical model of shunt formation, normal dogs developed anemia (Hct mean of 33%) and microcytosis (mean of 56 fL) within 18 weeks of creation of the shunt. Even though serum iron concentrations decreased, liver iron stores were increased suggesting a defect in iron metabolism (Laflamme et al 1994). Another study in 25 dogs with congenital shunts showed that MCV and MCHC were abnormal in around 60% of the dogs. Serum iron was low in 56% of dogs, whereas % saturation was low in only 20% (which is inconsistent with a true or absolute iron deficiency) and 62% of dogs had increased hepatic iron. Surgical correction of the shunt resulted in resolution of the MCV changes in some dogs (Simpson et al 1997). Note that even though dogs with shunts can have microcytic and hypochromic RBCs, hypochromasia is typically not evident in RBCs on blood smear examinations (in our experience). If we observe hypochromasia in RBCs, then absolute iron deficiency (low body iron stores) is likely occurring, which we attribute to gastrointestinal bleeding secondary to the shunt. A syndrome of idiopathic noncirrhotic portal hypertension has also been associated with microcytosis in dogs (Bunch et al 2001). In contrast, microcytosis has not been reported in cats with shunts (or other species, but shunts are very rare in species other than the dog).
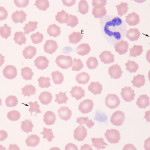
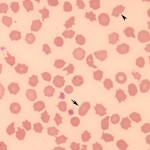
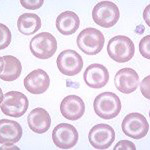
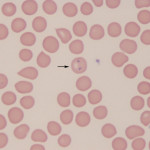
- RBC morphologic changes: Changes in RBC morphologic features occur in liver disease, but are not specific as to the cause of the disease. These changes are poikilocytosis, which includes acanthocytes and target cell formation. In both dogs and cats, acanthocytes can be a clue as to the presence of liver disease, but as for any RBC morphologic change, are not specific for liver disease. Cats with liver disease, particularly hepatic lipidosis, can develop many different shape changes, some of which defy naming, hence we often use the generic term of “poikilocytosis” in these animals. Again, poikilocytosis can be seen in cats without liver disease. Siderocytes may be seen in some dogs with shunts, supporting abnormal RBC turnover (which fits with increased hepatic iron stores). If dogs with liver disease (acute hepatitis, necrotizing hepatitis, cancer), secondary DIC can result in RBC changes, including acanthocytes, schistocytes and keratocytes. Some dogs with shunts can have RBC fragments (this is attributed to turbulent blood flow through the liver).
- Leukogram: This is generally normal in liver disease, unless there is inflammation or necrosis that recruits inflammatory cells, generating a systemic inflammatory response.
- Thrombogram: Even though thrombopoietin is produced in the liver, the platelet count is usually normal in animals with liver insufficiency, unless there is concurrent DIC.
|
|
|
|
|
Biochemistry panel
Naturally, the biochemical panel is key to identifying underlying liver disease, but results within reference intervals do not exclude the possibility of disease. Generally, we divide up the tests on a screening chemistry panel into “mini-panels” which allow us to detect the 4 main pathophysiologic processes:
- Hepatocellular injury: Increased activity of “leakage” enzymes – ALT, AST, SDH, GLDH. Some animals with hepatic injury may increased concentrations of unconjugated bilirubin and may develop cholestasis (with increased conjugated bilirubin) depending on the cause of the injury.
- Cholestasis: Increased activity of “inducible” enzymes – ALP, GGT – and concentrations of bilirubin (total and conjugated or direct, primarily). Cholestasis may secondarily result in hepatocellular injury due to toxic effects of bile or extension of the disease process from the portal region into the hepatic parenchyma. This will increase liver leakage enzymes and indirect bilirubin. If cholestasis is dominating, direct bilirubin is usually larger than indirect bilirubin concentrations, except in horses, in which direct bilirubin rarely dominates despite cholestasis.
- Hepatic insufficiency: Clues to this are obtained from the panel as none of the screening tests are definitive for hepatic insufficiency. Decreased concentrations of urea nitrogen, glucose, albumin, and cholesterol may be seen with liver insufficiency, but are not specific or sensitive to this condition. In fact, measurement of bile acids, ammonia and other proteins synthesized by the liver (antithrombin, protein C) are more sensitive to liver insufficiency than those tests on screening biochemistry panels.
- Abnormal blood flow: We often see mildly increased leakage enzyme (ALT, AST) and ALP activities in dogs with shunts, along with hemogram abnormalities (see above). Otherwise, we need to perform more specific tests of portal blood bypassing the liver, such as bile acids.
With respect to hepatocellular injury and cholestasis, it is useful to look at the degree of changes to see which pathophysiologic process is dominating. For instance, if increases in the inducible enzymes exceed that of the leakage enzymes, it suggests cholestasis or issues in the portal region or zone 3 of the liver is the dominant pathologic abnormality. In contrast, if liver leakage enzyme activities are very high, with mild to no increases in bilirubin, injury is dominating (and could be occurring anywhere in the liver). It is also worthwhile looking at other findings on a chemistry panel that may be responsible for the liver disease or arise because of liver disease. For instance, dogs and horses with chronic active hepatitis and cholangiohepatitis respectively, can have a polyclonal gammopathy (with increases in beta and gamma globulins) secondary to intestinal antigens not being metabolized by the liver and stimulating a generalized acquired immune response. Low iron and % saturation of transferrin may be seen in dogs with portosystemic shunts (see above). Horses with hypertriglyceridemia are at risk of developing hepatic lipidosis.

Urinalysis
Whenever possible, the urine should be examined in sick animals with suspected liver disease or to screen animals with an unknown condition. This is more readily accomplished in dogs and cats, where it is far easier to obtain urine than larger domestic species. The following abnormalities can be seen in urine with liver disease (but again are not specific for liver disease):
- Defects in concentrating ability: In hepatic insufficiency, decreased production of urea by a dysfunctional liver (>70-75% loss synthetic function ) will affect establishment of medullary hypertonicity and affect the ability of the kidney to concentrate urine, in the absence of renal disease. This may result in an inadequately concentrated urine when the kidney is asked to retain water (e.g. hypovolemia).
- Dipstick abnormalities: The most important abnormality is a positive reaction for bilirubin on the dipstick (that is confirmed by tablet versions of the test if the color reaction is weak or the urine is strongly colored). Bilirubin in the urine must be water soluble so bilirubinuria is due to conjugated or direct bilirubin. Thus, in all species other than the dog and the ferret, bilirubinuria is abnormal and indicative cholestasis with increases in direct bilirubin in blood. In fact a biilrubinuria usually precedes bilirubinemia in early cholestasis as the kidney excretes the excess direct bilirubin, lowering values in blood. Dogs, particularly male dogs, can have a 1+ reaction for bilirubin (and rarely up to 2+) in concentrated urine (>1.030 USG), but a 1+ bilirubinuria in dilute urine (USG < 1.008) would be clearly abnormal (as would a 3+ bilirubinuria in concentrated urine) and indicate excessive bilirubinuria and underlying cholestasis. Ferrets are reported to have small amounts of bilirubin in the urine (unknown cause) (Orcutt 2003).
- Crystals: Ammonium biurate crystals can form in the urine in dogs and cats with portosystemic shunts due to decreased metabolism with subsequent high serum concentrations of ammonia. They can also be seen in certain dog breeds, e.g. Dalmatians, with inherited defects in urate metabolism.
- Acquired Fanconi syndrome: Dogs with hepatic copper accumulation, secondary to genetic defects in copper metabolism (e.g. COMMD1 or ATBP7 in Bedlington Terriers [Forman et al 2005, Coronado et al 2008]) or genetic predisposition to copper accumulation (e.g. Labrador Retrievers [Dirksen et al 2017]) can also accumulate copper in renal tubules (mostly proximal but also distal). Renal tubular accumulation of copper can injure the tubules resulting in acquired Fanconi syndrome or proximal renal tubular dysfunction (Langlois et al 2013). The dysfunctional tubules cannot readily resorb normal filtered substances such as amino acids (protein), glucose, ketones, or bicarbonate, leading to proteinuria excessive for the urine specific gravity, ketonuria without ketonemia or excess ketone production, glucosuria in the absence of hyperglycemia and bicarbonaturia. Patients can have a hyperchloremic (normal anion gap) metabolic acidosis due to the inability to reabsorb filtered bicarbonate (hence ammonium chloride is retained by the proximal tubules and acidifies blood) and can have an alkaline urinary pH, however the distal tubules are often still functional and can excrete acid via H-ATPases in the type A intercalated cells. So the urine may have a normal pH or even be acidic. Distal tubular excretion of acid prevents the primary metabolic acidosis due to excess bicarbonate excretion from becoming too severe, unless the distal tubules are dysfunctional as well, which can be seen in dogs with copper accumulation. Affected dogs have hepatic disease, including liver injury (increased ALT activity), cholestasis (increased ALP activity, total bilirubin concentrations and bilirubinuria) and dysfunction (increased ammonia concentrations, prolonged coagulation times). Some are concurrently azotemic with isosthenuric urine, suggesting that distal tubules are dysfunctional due to copper (which may also explain alkaline urine in some dogs, if they can no longer acidify the urine). On histopathologic examination, copper accumulation is seen primarily in proximal tubules but also affects the other tubules. Proximal renal tubular necrosis, usually acute, is present, but there is also evidence of tubulointerstitial nephritis, which may affect overall renal function, resulting in the concurrent azotemia and contributing to the distal tubular defects (Langlois et al 2013).
Coagulation tests
Since hepatocytes produces most of the coagulation factors (exception being factor VIII, which is produced in hepatic sinusoidal and extrahepatic endothelial cells), synthetic liver failure (>70-75% loss of liver) can result in a hemorrhagic diathesis. The liver also produces coagulation inhibitors (antithrombin, protein C, protein S etc), but we really do not recognize thrombosis in animals as a consequence of hepatic insufficiency (probably just because it is difficult to detect thrombosis generally as some human patients with liver dysfunction do suffer from thrombosis), although measurement of antithrombin and protein C are good markers of hepatic insufficiency or failure as well as portosystemic shunting (protein C). For more on how the liver affects hemostasis, refer to the hemostasis section of the website.
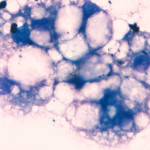
Cytology
Naturally aspiration of the liver can yield definitive diagnosis with diffuse liver disease (e.g. hepatic lipidosis or lymphoma). Liver disease (particularly chronic or diseases associated with portal hypertension) can also result in ascites, which is typically a transudative effusion. Examination of abdominal fluid can occasionally yield a definitive diagnosis as to the cause of liver disease, e.g. exfoliating neoplasia. For more on effusions, see the cytology section of the website.