
Changes in red blood cell (RBC) size on a blood smear correspond to changes in diameter of the cell and not necessarily to changes in red blood cell volume, as assessed by the hematologic analyzer. Cells can appear smaller but be of normal volume (e.g. spherocytes) whereas other cells actually appear bigger because they are thinner and spread more in a blood smear (hypochromic red blood cells). Variation in red blood cell size on a blood smear is called anisocytosis and this can be due to increased proportions of larger red blood cells than normal, smaller red blood cells than normal or a combination of both. Thus, anisocytosis has no more specific meaning other than increased variation in red blood cell size (diameter). Note that low numbers of larger or smaller red blood cells may not increase or decrease the mean cell volume (MCV) above or below reference limits. There needs to be sufficient numbers of cells of higher or lower volume to shift the mean volume. Modern hematology analyzers also measure the variation in red blood cell volume and report this value out as a red blood cell distribution width (RDW). This does correlate somewhat to the smear examination assessment of anisocytosis. At Cornell University, we only report macrocytes, when they are distinctly visualized in a blood smear. These may or may not be associated with a macrocytosis (MCV higher than the upper reference limit), depending on the numbers in blood. We do not report microcytes, because they are of uncertain diagnostic relevance. However, microcytosis (MCV below the lower reference limit) can be a physiologic or pathologic finding in animals. Thus, only macrocytes will be discussed here.
Macrocytes
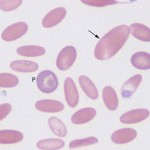
These are larger red blood cells than normal. Macrocytes have a normal content of hemoglobin and very little RNA. In fact, there is insufficient RNA (blue) to offset the red of hemoglobin, so macrocytes are red in color. This differs from polychromatophilic RBC which are usually larger and purple because they contain more RNA. Detection of macrocytes requires the presence of cells of normal size in the blood. If all the cells are macrocytic, it is difficult to recognize that they are larger than normal (i.e. there is nothing to compare them to).
Macrocytes form through several mechanisms:
- Regeneration: Macrocytes can be (but are not always) younger RBC than normal. They can be seen in all mammalian species that are mounting a regenerative response. Indeed, these are the cells we look for in an anemic horse to assess whether the horse is responding to the anemia (or not). This is because equine release only low numbers of reticulocytes in response to an anemia. These can be counted by modern hematology analyzers (using fluorescent dyes) but are not usually detectable as polychromatophilic RBC in blood. Immature macrocytic RBC will probably contain small amounts of RNA, which is precipitated by vital dyes, such as new methylene blue, or binds fluorescent dyes, such as oxazine, i.e. they are usually punctate reticulocytes. Punctate reticulocytes have a 3 day half life in cats (they can persist in blood for 7-10 days). Cats that have recovered from an anemia may be macrocytic due to persistence of this punctate reticulocytes (post-regenerative macrocytosis). Premature release of RBC may underly macrocytosis seen in some animals with hyperthyroidism.
- Abnormal DNA synthesis: Since RBC becomes successively smaller with each cell division during erythropoiesis, larger RBC are formed if DNA synthesis is retarded or abnormal. This occurs under the following situations:
- Feline leukemia virus (FeLV) infection: The virus integrates into the feline host cell genome and retards DNA metabolism. The virus also causes neoplastic transformation of feline erythroid cells, called primary myelodysplasia. Macrocytosis is a characteristic feature of myelodysplastic syndrome in the cat and is frequently seen in the presence of a severe non-regenerative anemia.
- Myelodysplasia: Abnormal production of red blood cells can result in macrocytosis. This is most frequently seen in cats with FeLV infection and rarely in other species.
- Congenital dyserythropoiesis: Congenital dyserythropoietic anemia (CDA) is an inherited defect in humans that results in macrocytosis. This has been reported in Poll Hereford cattle and is likely the cause of macrocytosis in Poodles (despite the lack of anemia).
- Mineral/nutrient deficiencies: Vitamin B12, cobalt and folate are required for DNA synthesis (purine and pyrimidine metabolism or synthesis of nucleic acids). Deficiencies in these vitamins and minerals can result in macrocytosis, with or without anemia. Molybdenum excess in pastures or feed can result in a secondary cobalt deficiency in ruminants.
- Drugs: Drugs which interfere with vitamin B12 metabolism or folate absorption can result in macrocytosis (with or without anemia), e.g. hydroxyurea, sulfur drugs.
- Red blood cell swelling: This can occur due to membrane defects (e.g. hereditary stomatocytosis), hyperosmolality (e.g. diabetes mellitus) or a storage-associated artifact. Since this affects all RBC, macrocytes are usually not identified readily on the blood smears, although the MCV may be above the upper reference limit for that species.