
Impression smears from an adrenal gland mass of a dog
Case information
A 9-year-old, male castrated Lhasa apso was presented to the ophthalmology service for surgical removal of diabetic cataracts. The dog was diagnosed with diabetes mellitus 8 months ago and has been maintained on Novalin-N insulin. The dog had developed bilateral cataracts two months previously and had shown vision impairment. Prior to surgery, screening blood work was performed. The complete blood count was within normal limits and a chemistry panel revealed mild hyperglycemia (181 mg/dl, reference interval: 63-118 mg/dl), mildly increased alkaline phosphatase activity (200 U/L reference interval: 17-111 U/L), moderate to marked hypercholesterolemia (554 mg/dL, reference interval: 138-332 U/L), and moderate hypertriglyceridemia (408 mg/dL, reference interval: 22-125 mg/dL). During surgery, the dog had self-limiting, spontaneous bouts of severe systemic hypertension (systolic blood pressure of 300 mmHg), but recovered uneventfully.
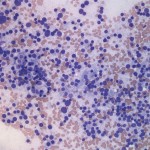
The dog was presented for further evaluation of intermittent systemic hypertension and ocular recheck two weeks after surgery. The systemic blood pressure was mildly increased (159/117 mmHg with a mean arterial pressure of 133 mmHg). Abdominal ultrasound revealed a 2.7 cm x 1.9 cm, hyperechoic mass on the right adrenal gland with evidence of adjacent vascular invasion and tumor thrombus. The left adrenal gland was normal in size. Given the lack of distant metastasis, right adrenalectomy was performed. Touch impression smears of the adrenal gland mass were made for cytologic evaluation.
- Based on the clinical presentation, what would be your top differential diagnosis for the adrenal mass?
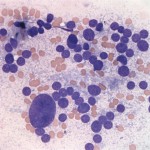
- How would you classify the cell population (epithelial, mesenchymal, round, or endocrine/neuroendocrine) in Figures 1 and 2?
- What cellular criteria of malignancy can you appreciate in Figure 2?
 |
 |
Answer on next page