
Aspirate of a mass at the thoracic inlet of a 30 year old hypercalcemic horse
Case Information
A 30 year old Quarter Horse gelding was presented to the Nemo Farm Animal Clinic at Cornell University’s Hospital for Animals for a dental examination. The horse had been previously diagnosed 1 month prior with pars pituitary intermedia dysfunction (PPID) and was being treated with pergolide. The gelding had lost a substantial amount of weight over the winter and had a reduced appetite. A dental examination revealed resorption of incisors and severely worn cheek teeth. On physical examination, the gelding had a 2/9 body condition score. He was bright, euhydrated and had a long, unkempt, and greasy haircoat. Muscle atrophy was severe and a mild systolic murmur was detected on thoracic auscultation. The dental disease was not judged severe enough to result in the severe weight loss or inappetence, thus clinical pathologic testing was performed.
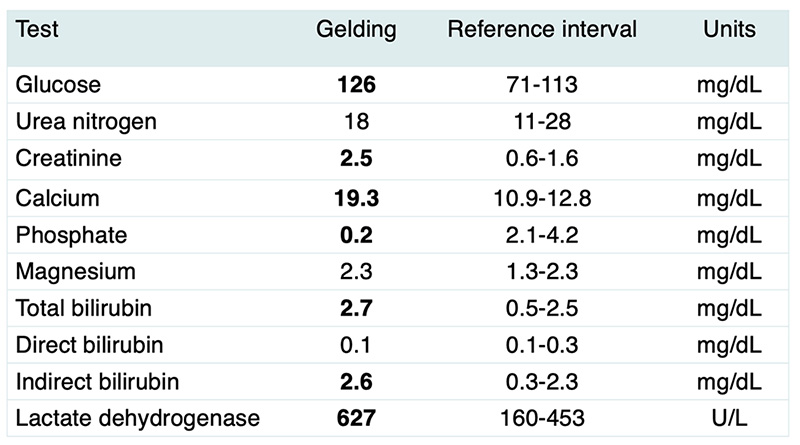
Hemogram results were within normal limits. Abnormal serum chemistry results are shown in the table below (not stated results were normal) and the sample was not hemolyzed or lipemic. The sample was mildly icteric, commensurate with the mildly increased total bilirubin concentration. A voided urine sample was collected and had a specific gravity of 1.009 and a pH of 8.0 units. No other abnormalities were noted on the urine dipstick or sediment examination.
- At this stage, what are your differential diagnoses for hypercalcemia in horses?
- What additional tests would you perform to rule in or out your differential diagnoses?
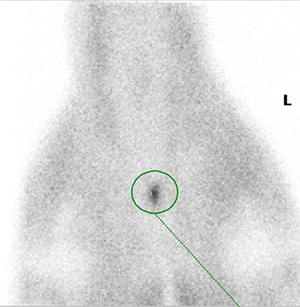
Based on the chemistry results, imaging was performed. Gastric endoscopy showed no stomach lesions. Thoracic ultrasonographic examination revealed diffuse mild to moderate comet tailing, supporting underlying inflammation, and a small nodule in the right caudodorsal lung. A 2 x 1 cm hyperechoic round mass was identified in the midline of the thoracic inlet and both thyroid glands contained small hypoechoic nodules at the cranial ends. The right thyroid gland was larger than the left gland. Additional small hypoechoic nodules were found along the neck and were larger on the right side (presumptive lymph nodes). Assessment of the abdomen did not reveal any abnormalities. Thoracic radiographic examination revealed a heterogeneous poorly defined 20 x 30 cm lesion in the region of the cranial mediastinum of the left hemithorax. Blood was submitted to the University of Michigan for a hypercalcemia malignancy panel, consisting of ionized calcium, parathyroid hormone (PTH) and parathyroid hormone-related peptide (PTHrP). Nuclear scintigraphy was performed and showed normal radioactive tracer uptake in the thyroid and salivary glands but increased uptake in the mass at the thoracic inlet (Figure 1, green circle).
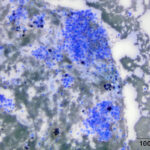
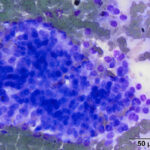
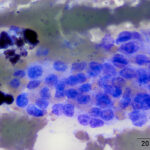
The horse was treated with intravenous fluids, which decreased the creatinine concentration to 1.9 mg/dL. Surgical resection of the mass was performed 2 months later. While under anesthesia, the mass was aspirated and direct smears of the aspirate were submitted for cytologic examination. View the provided cytologic images then answer the questions below.
- Based on the cells in the aspirate, what is your diagnosis?
- Based on all the results taken together, what is the likely origin of the mass?
 |
 |
 |
Answers on next page