
A Cat with a Renal Mass
Case Information
A 13-yr old female spayed domestic longhair cat presented to the oncology service at Cornell University Hospital for Animals for a renal tumor. The cat presented to the regular veterinarian with a 2-week history of progressive hyporexia, suspected weight loss and intermittent vomiting. On physical examination by regular veterinarian, the cat was noted to have bilateral renal enlargement, hypercalcemia and azotemia. At that time, renal neoplasia was discussed and supportive care was provided. Vomiting resolved with supportive care, but the cat continued to be progressively anorectic and continued to lose weight.
On presentation to Cornell, the cat’s temperature, respiration and heart rate were within normal limits. The cat was quiet, but alert and responsive, with a body condition score of 3/9 (cachectic). On abdominal palpation the right and left kidneys were moderately and mildly enlarged, respectively. A complete blood count revealed a mild normocytic normochromic non-regenerative anemia (RBC 6.5 mill/uL [reference interval 6.9-10.1 mill/uL]; MCV 48 fL [reference interval 40 – 52 fL]; MCHC 33 g/dL [reference interval 32 – 35 g/dL]), consistent with anemia of chronic disease, and a moderate thrombocytopenia (92 thou/uL [reference interval 195-624 thou/uL]). Serum biochemical testing revealed a moderate azotemia (urea nitrogen 74 mg/dL [reference interval 16 – 36 mg/dL]; creatinine 1.8 mg/dL [reference interval 0.6 – 2.0 mg/dL]) interpreted as a renal azotemia, moderate hypercalcemia (16.4 mg/dL [reference interval 9.1-10.9 mg/dL]) with a moderate increase in ionized calcium (2.25 mmol/L [reference interval 1.11-1.38 mmol/L] with a concurrent mild hypophosphatemia (2.6 mg/dL [reference interval 2.7-6.2 mg/dL]), mild proportional hyponatremia and hypochloremia (sodium 150 mEq/L [reference interval 151 – 158 mEq/L]; chloride 112 mEq/L [reference interval 113 – 123 mEq/L]), interpreted as fluid losses (likely renal) with water replenishment through drinking. There was mild evidence of muscle injury (creatine kinase 735 U/L [reference interval 73 – 388 U/L] and AST 65 U/L [reference interval 15 – 44 U/L]). Concurrent liver injury could not be ruled out, particularly as the cat had very mildly alkaline phosphatase activity (85 U/L [reference interval 13 – 83 U/L]).
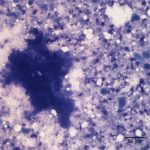
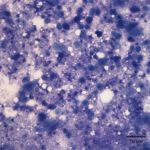
Abdominal ultrasound revealed a mass in the right kidney and extending into renal vessels, that was lobulated and heterogeneous. A fine needle aspirate of the mass was performed. Evaluate the photomicrographs of the fine needle aspirate and answer the following questions:
 |
 |
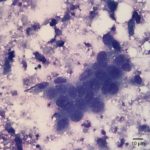 |
- What uncommon findings are present in the fine needle aspirate of the renal mass?
- How would the hypercalcemia be explained in this case?
Answer on next page