
Interpretation
Canine Granulocytic Ehrlichiosis (anaplasmosis)
Explanation
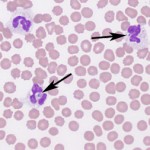
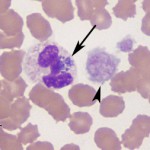
In both images, basophilic cytoplasmic inclusions are seen in neutrophils (arrows in images below); these inclusions are morulae, which are observed during acute infection with Anaplasma phagocytophilum or Ehrlichia ewingii, the agents of granulocytic ehrlichiosis. Morulae were seen in moderate numbers of neutrophils in this patient’s blood smear. Thrombocytopenia is the most common hematologic abnormality in dogs with granulocytic ehrlichiosis1 and this diagnosis explains the thrombocytopenia observed in the patient. The thrombocytopenia in this case is moderate to severe and, although spontaneous bleeding often does not occur until the platelet count drops below 30,000/uL,2 platelet function defects have been recognized in acute canine ehrlichiosis.3 The thrombocytopenia, along with possible decreased function of the remaining platelets, is likely responsible for the hematochezia noted on physical exam. The mild anemia (which was normocytic normochromic) is consistent with anemia of inflammatory disease although gastrointestinal blood loss could be contributing in this case. The observed lymphopenia and eosinopenia were likely a result of stress associated release of endogenous corticosteroids. All of these changes have been described in other cases of canine granulocytic anaplasmosis.1
 |
 |
Discussion
Epidemiology
Canine and human granulocytic ehrlichiosis are caused by Anaplasma phagocytophilum and Ehrlichia ewingii, both of which are obligate intracellular bacteria belonging to the order Rickettsiales. Both agents are tickborne; A. phagocytophilum and E. ewingii are transmitted by Ixodes species (black-legged tick) and Amblyomma amercianum (lone star tick), respectively. The primary reservoir hosts are deer (E. ewingii) and rodents (A. phagocytophilum). Based on surveys of serological assays in the USA, Anaplasma species are most prevalent in the Northeast, Midwest and in California, whereas Ehrlichia species are most prevalent in the Southern states.4
Pathogenesis
A. phagocytophilum is transmitted 36-48 hours after attachment of the tick vector to its host;5 the attachment time required for transmission of E. ewingii is unknown. Following transmission, the agents primarily infect neutrophils. Phagocytic and bactericidal function is diminished in infected neutrophils, thereby increasing host susceptibility to other bacterial infections. Ultimately, the host develops adequate cell-mediated and humoral immunity, allowing clinically affected dogs to recover following acute disease, however it is unclear whether or not dogs can remain persistently infected.6,7
Clinical Features
Infection usually results in subclinical disease.5 When clinical signs do occur, they appear one to two weeks post-infection. Common clinical signs are fever, lethargy, inappetance and lameness, as well as hemorrhage in some cases. Neurological signs (head tilt, tremors and anisocoria) have been observed in dogs infected with E. ewingii. Although mild anemia, leukopenia and increased serum alkaline phosphatase activity are common clinicopathologic findings, the most prominent laboratory anomaly is thrombocytopenia.1 Several mechanisms have been proposed for the underlying pathophysiology of the thrombocytopenia, including immune-mediated platelet destruction and splenic sequestration of platelets, however studies have refuted these theories; the underlying mechanism remains unclear and likely represent multiple immunologic and non-immunological mechanisms.8,9 The macroplatelets observed in the blood smear of this patient (see Figure 4 above), along with the increased mean platelet volume (MPV), suggest increased production of platelets by the bone marrow, supporting peripheral causes for the thrombocytopenia.
Diagnosis
Several diagnostic tests are available for granulocytic ehrlichiosis (see Table 2), however, these tests must be interpreted in light of the clinical signs displayed by the patient and with knowledge of the individual tests and the progression of positive results during active infections.
| Table 2: Diagnostic evaluation and select clinical findings for canine granulocytic ehrlichiosis/anaplasmosis | |
| Test | Time of appearancea |
| Blood smear examination for morulae in neutrophils | Seen 4-14 days post-inoculation |
| Polymerase chain reaction for bacterial DNA | Seen a few days before morulae and may persist for a few days after morulae are undetectable |
| Clinical signs (fever) and hematologic findings (thrombocytopenia) | Occurs 4-14 days post-inoculation |
| Serologic testing Immunofluorescent antibody (IFA) and 4Dx Plus SNAPb |
Positive 2-5 days after appearance of morulae in neutrophils |
| a Based on experimental infection of 7 dogs with E. ewingii.10 Other experimental studies have demonstrated a similar sequence of appearance of clinical signs and detection of infection, though variation in the days post inoculation is seen between studies.7,11 b IDEXX, Westbrook, ME |
|
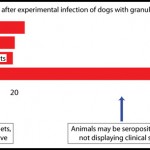
Figure 5 roughly illustrates the relative sequence of events, based on one study of experimental infection of 7 dogs with granulocytic ehrlichiosis.10 This figure illustrates the pitfalls in relying on serologic testing alone since seroconversion is often seen several days after animals display clinical signs. Since morulae can be detected within neutrophils shortly before seroconversion, as was observed in our patient in which the 4Dx Plus SNAP test was negative, the examination of a freshly prepared blood smear is a valuable diagnostic tool. Furthermore, antibodies can persist for several months after resolution of acute illness. For these reasons, a negative antibody test does not rule-out granulocytic ehrlichiosis or anaplasmosis in an acutely ill dog and a positive serology test does not necessarily imply current infection with these agents. Polymerase chain reaction (PCR) is often the earliest marker for disease and should be considered in patients for which there is a high index of suspicion but other testing (including examination of a blood smear) is negative. PCR testing is also the only diagnostic test that distinguishes between A. phagocytophilum and E. ewingii infections. Click here for more information on diagnostic testing for these diseases at Cornell University or refer to the Animal Health Diagnostic Center website.
Treatment and prevention
Doxycycline is the treatment of choice (10 mg/kg PO daily for four weeks). Although a two-week course of treatment reliably clears A. phagocytophilum and E. ewingii, a four-week course is recommended due to the likelihood of concurrent tickborne disease, such as Lyme borreliosis (also transmitted by Ixodid ticks). Visible ticks should be removed promptly and an acaricidal product (fipronil, permethrin, deltamethrin, amitraz, selamectin, etc.) should be applied to the dog year-round.12
Further information and follow-up
Antimicrobial therapy with intravenous doxycycline was initiated. On the following day, the patient’s energy level and appetite improved. Complete blood count revealed a mild lymphocytosis (4.9 thou/μL) and thrombocytopenia (28 thou/μL) with platelet clumping. No morulae were seen in the blood smear. The patient’s overall condition continued to improve over the next 24 hours. Another blood smear was examined and showed increased numbers of platelets (estimated at 5 per 1000x oil magnification field, corresponding to an approximate count of 75 thou/μL). The patient was prescribed a 4-week course of oral doxycycline and was discharged to the care of the owners. The following week, the dog returned for a recheck examination. Physical examination revealed no abnormalities; there was no external evidence of hemorrhage. The CBC and blood smear analyses revealed persistent mild anemia (hematocrit of 39%), however the platelet count had normalized (279 thou/μL) and no morulae were seen in neutrophils. Doxycycline therapy was continued as prescribed and the owner was advised to apply an ascaricidal product year-round.
References
- Kohn B, Galke D, Beelitz P, Pfister K. Clinical features of canine granulocytic anaplasmosis in 18 naturally infected dogs. J Vet Intern Med 2008 Nov-Dec;22(6):1289-1295.
- Stockham SL. Fundamentals of veterinary clinical pathology. 2nd ed. ed. Ames, Iowa: Blackwell Pub.; 2008.
- Harrus S, Waner T, Eldor A, Zwang E, Bark H. Platelet dysfunction associated with experimental acute canine ehrlichiosis. Vet Rec 1996 Sep 21;139(12):290-293.
- Little SE. Ehrlichiosis and anaplasmosis in dogs and cats. Vet Clin North Am Small Anim Pract 2010 Nov;40(6):1121-1140.
- Carrade DD, Foley JE, Borjesson DL, Sykes JE. Canine granulocytic anaplasmosis: a review. J Vet Intern Med 2009 Nov-Dec;23(6):1129-1141.
- Munderloh UG, Lynch MJ, Herron MJ, Palmer AT, Kurtti TJ, Nelson RD, et al. Infection of endothelial cells with Anaplasma marginale and A. phagocytophilum. Vet Microbiol 2004 Jun 10;101(1):53-64.
- Yabsley MJ, Adams DS, O’Connor TP, Chandrashekar R, Little SE. Experimental primary and secondary infections of domestic dogs with Ehrlichia ewingii. Vet Microbiol 2011 Jun 2;150(3-4):315-321.
- Borjesson DL, Simon SI, Tablin F, Barthold SW. Thrombocytopenia in a mouse model of human granulocytic ehrlichiosis. J Infect Dis 2001 Dec 1;184(11):1475-1479.
- Granick JL, Reneer DV, Carlyon JA, Borjesson DL. Anaplasma phagocytophilum infects cells of the megakaryocytic lineage through sialylated ligands but fails to alter platelet production. J Med Microbiol 2008 Apr;57(Pt 4):416-423.
- Egenvall A, Bjoersdorff A, Lilliehook I, Olsson Engvall E, Karlstam E, Artursson K, et al. Early manifestations of granulocytic ehrlichiosis in dogs inoculated experimentally with a Swedish Ehrlichia species isolate. Vet Rec 1998 Oct 10;143(15):412-417.
- Stockham SL, Tyler JW, Schmidt DA, Curtis KS. Experimental transmission of granulocytic ehrlichial organisms in dogs. Vet Clin Pathol 1990;19(4):99-104.
- Neer TM, Breitschwerdt EB, Greene RT, Lappin MR. Consensus statement on ehrlichial disease of small animals from the infectious disease study group of the ACVIM. American College of Veterinary Internal Medicine. J Vet Intern Med 2002 May-Jun;16(3):309-315.