
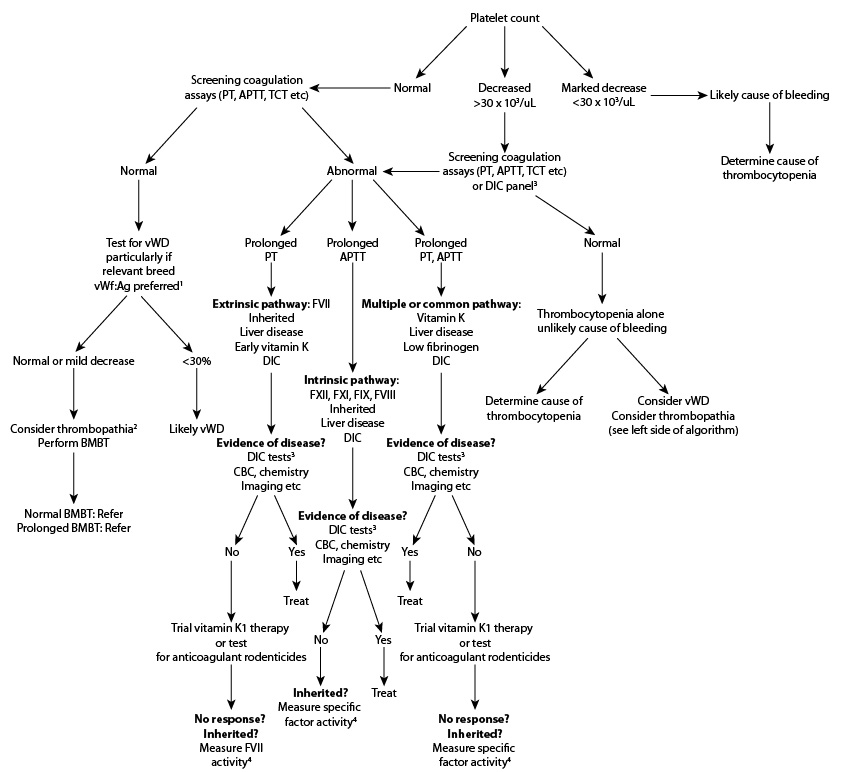
1 Genetic testing for vWD can be done in those breeds for which a genetic test is available, however the genetic test does not necessarily correlate to clinical signs.
1 Thrombopathia (decreased platelet function) is uncommon as a cause of hemorrhage, but can be inherited or secondary to drugs (e.g. aspirin, non-steroidal anti-inflammatory drugs), disease (uremia, liver disease, DIC). A complete medical history, including drug administration or exposure to toxins, is imperative in bleeding animals.
3 Perform additional assays for DIC testing as required, e.g. fibrinogen concentration, FDP/D-dimer concentration, AT activity. Note: If there is a high clinical suspicion of DIC (sick animal with underlying predisposing disease, e.g. bacterial sepsis, cancer, severe inflammation, immune-mediated hemolytic anaemia), consider concurrent DIC panel and platelet count (versus sequential testing as illustrated). Furthermore, in areas where Angiostrongylus vasorum is a problem, testing for this worm that resides in the heart and pulmonary arteries (PCR, ELISA, fecal flotation) is advisable and empirical treatment may be worthwhile.
4 Measurement of FVIIa activity is being used by some clinicians as a marker of vitamin K deficiency, in preference to the PIVKA (proteins induced by vitamin K absence or antagonism) test. Note: Vitamin K deficiency can be due to toxicosis, fat malabsorptive disorders, or liver disease (e.g. cholestatic disorders).
“Reproduced and modified with permission from the BSAVA Manual of Canine and Feline Clinical Pathology, 3rd edition.”