
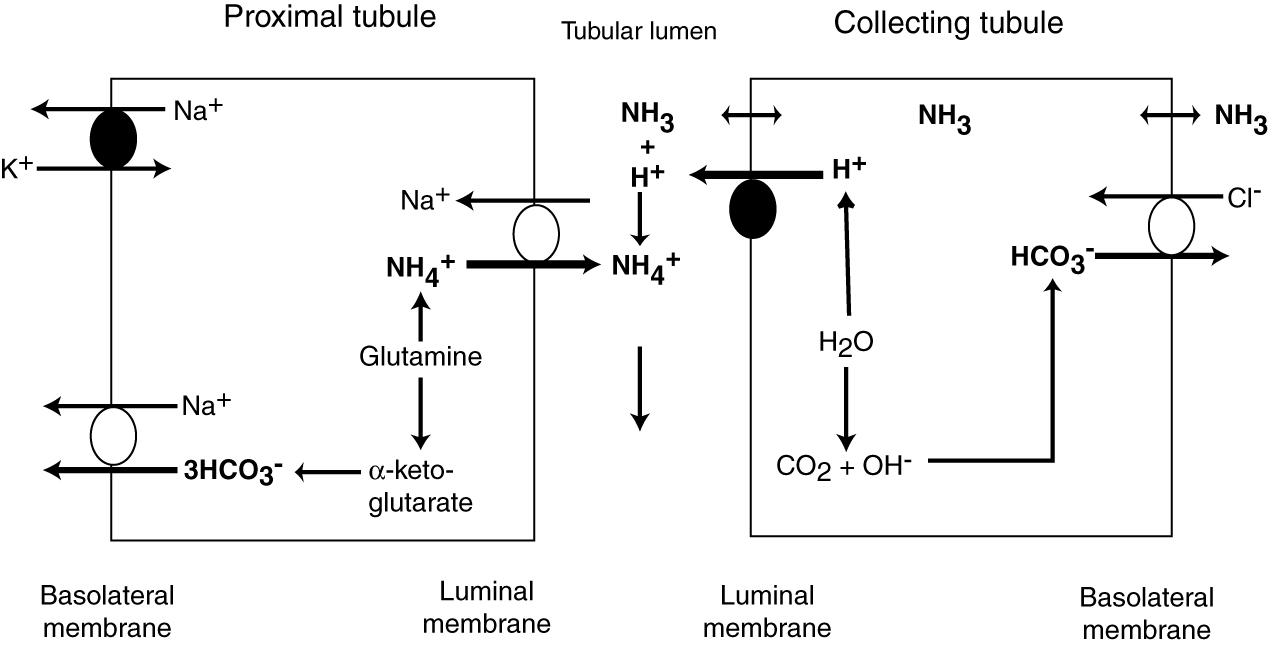
The kidney is capable of excreting acid (as ammonium chloride) and generating new bicarbonate (not just reclaiming filtered bicarbonate), when it produces ammonium from glutamine (amino acid). This is the way the kidney can generate bicarbonate and excrete hydrogen in acidemic or acidotic states and how it can decrease acid excretion (and promote bicarbonate loss) in alkalemic/alkalotic states. In the proximal tubules, ammonia generation is linked to sodium absorption whereas in the distal tubules it is linked to hydrogen excretion (with chloride).
1) In the proximal tubule, ammonium (NH4+) is generated from glutamine. The ammonium is transported into the renal lumen in exchange for sodium by a luminal exchanger. The ammonium is then “lost” or excreted into the urine with chloride as its anion (not shown). This generates new bicarbonate (via glutamine metabolism), while excreting an acid (ammonium chloride).The bicarbonate is returned to the blood via the basolateral sodium/bicarbonate cotransporter, which derives its energy from a basolateral sodium/potassium exchanger or pump. Hypokalemia and acidemia stimulates ammoniagenesis, promoting hydrogen excretion and bicarbonate retention. Angiotensin II stimulates the basolateral sodium/bicarbonate cotransporter, facilitating absorption of the generated bicarbonate.
2) In the collecting tubule, ammonia (NH3) diffuses freely across the renal tubular cell and combines with hydrogen excreted by the H+ATPase. Chloride passively follows (brought into the cell in exchange for bicarbonate which is resorbed by the basolateral chloride/bicarbonate exchanger). The hydrogen ATPase pump on the luminal surface and the basolateral chloride/bicarbonate exchanger are stimulated by aldosterone.
In both tubules, excretion of hydrogen is linked to generation of new bicarbonate.