
Interpretation
Mesenchymal tumor, likely meningioma
Explanation
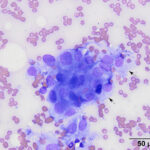
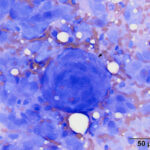
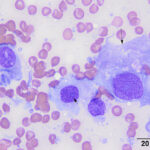
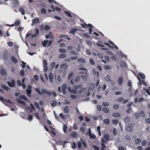
The aspirate was highly cellular, consisting of large numbers of tissue cells on a background of a moderate amount of blood. The tissue cells were seen individually and in aggregates and whorls (Figures 1-3). The cells were spindled to polygonal and contained paracentral nuclei within a moderate amount of light blue cytoplasm with indistinct borders, which were frequently wispy (Figures 2, 4). The nuclei were round to oval with coarsely stippled chromatin and usually contained a single indistinct nucleolus. Anisocytosis and anisokaryosis were mild, but scattered cells with larger nuclei, along with rare binucleated cells, were seen. The cytologic features were consistent with a mesenchymal tumor and, based on location, likely a meningioma (Question 1). Biopsy with histopathologic examination would be required to confirm this diagnosis (Question 2).
|
|
|
|
Additional tests
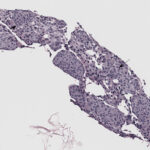
A Tru-cut biopsy with histopathologic examination was performed to confirm a diagnosis of meningioma. The mass was cellular and comprised of a population of spindled to polygonal cells, arranged in circular and whorl-like aggregates, supported by a fine fibrovascular stroma. The cells had indistinct borders with a moderate amount of light amphophilic cytoplasm, and round to oval to elongate central to eccentric nuclei, with finely stippled to vesicular chromatin, and single small nucleoli. The cells displayed mild anisocytosis and anisokaryosis and no mitotic figures were identified in the biopsy sections. The histologic findings were consistent with a retrobulbar or orbital meningioma, with the cellular features suggesting a grade I out of III meningothelial subtype, based on the World Health Organization (WHO) International Histological Classification of Tumors of Domestic Animals.1
|
|
|
A CBC and biochemical profile, abdominal ultrasonographic examination and thoracic radiographs were performed to evaluate for systemic disease and/or metastasis. The CBC showed a lymphopenia (0.7 thou/μL; reference interval, 0.9-4.7 thou/μL), which could be due to endogenous corticosteroids (stress) or prior corticosteroid therapy (noted in the history). The biochemical profile showed increased ALP (1688 U/L; reference interval, 7-155 U/L) and CK (705 U/L; reference interval, 64-314 U/L) activities. The increased ALP activity may be due to stress and the previous steroid therapy, although other causes could not ruled out. The mildly increased CK activity could be due to a “muscle stick” or mild muscle injury, which was not clinically relevant. There was no evidence of metastatic disease, with only a nodular hepatopathy being detected on ultrasonographic examination (the latter could be due to nodular hyperplasia).
Discussion
Meningiomas arise from meningothelial or arachnoid cells of the meninges. They usually form expansile intradural lesions that compress and frequently invade into underlying parenchymal tissue in dogs, but are less invasive in cats.1,2 They are the most frequently occurring primary neoplasms of the central nervous system in dogs, usually arising within the brain. The most common location is in the olfactory bulb, comprising around 1/3 of all meningiomas.2-5 Less commonly, they can be found in other sites, such as the spinal cord and retrobulbar space.3,5 Orbital (retrobulbar) meningiomas can be primary tumors, when meningeal (arachnoid cap) cells undergo neoplastic transformation within the optic nerve sheath. They can also occur from secondary extension of an intracranial neoplasm along the optic nerve.3 In dogs, primary orbital meningiomas are usually low-grade slow growing benign tumors. However, cases of intraocular, muscle and fat invasion and malignant forms with metastasis have been reported.3,5 Clinical signs frequently observed in dogs with retrobulbar meningiomas include exophthalmos, orbital swelling, prolapsed globes, and blindness,3,6 similar to that described for the case presented herein. Fundic abnormalities, such as papilledema, abnormal optic disks, and retinal hemorrhage, can also be seen.3 In one study of 22 retrobulbar meningiomas in dogs, Poodles, Samoyeds, and German shepherds or their crosses were the most commonly affected breeds and dogs were older (mean age at the time of diagnosis, nine years old, range, 3-17 years) and mostly males (13/20 cases).2
Diagnostic tests for suspect orbital meningiomas may include imaging studies, including ultrasonographic, CT, or magnetic resonance imaging, to provide clinical details of the eye and related structures. Cytological examination of a fine needle aspirate of the lesion can also be useful in identifying neoplastic cells. Smears of aspirates often contain spindle-shaped cells, which may be organized in large whorling structures, as seen in this case.6-9 However, more polygonal (epithelioid) variants with pink-red cytoplasmic granules may be observed.1,2,6,9,10 Although a presumptive diagnosis of meningioma can be made from cytologic assessment of retrobulbar masses, a definitive diagnosis requires histopathologic examination.
On gross appearance, retrobulbar meningiomas form cone-shaped solid masses, which adhere to the posterior aspect of the globe and encircle the optic nerve.3,5 Meningiomas can be classified into 9 subgroups according to their features in histologic sections, using the WHO system for animals:1,2 Meningothelial (polygonal cells forming solid lobules), fibroblastic (spindled cells forming fascicles), transitional (mixed solid and fibroblastic, which often has whorling arrangements, usually around vessels), psammomatous (has psammoma bodies in the center of hyalinized aggregates or whorls), angiomatous, papillary, granular cell (contains periodic-acid schiff positive granules that are resistant to diastase), myxoid, and anaplastic (hasfeatures of malignancy, including a high mitotic rate and invasion).1,2 Additional subtypes are described in humans11 and dogs, including microcystic and metaplastic variants.2,12 The human WHO classification scheme also grades meningiomas as to their anticipated biological behavior from I (benign) to II and III (more metastatic or locally aggressive).11 Grade III meningiomas have features of malignancy (pleomorphism, high mitotic rate, invasion).2 Canine retrobulbar meningiomas are usually meningothelial with fewer transitional or granular types and can have multiple foci of myxoid, osseous or chondroid metaplasia.3,5,6,10 They are classified as grade I neoplasms by the WHO and tend to show recurrence or local invasion along the optic nerve if not completely resected.3 For the patient in this case, cellular features supported a grade I out of III meningothelial subtype, although the whorling arrangements are more characteristic of the transitional type (the biopsy was small and the fibrous component of the biopsy may have been missed). There are no unique immunohistochemical markers for meningiomas, but they typically stain strongly for vimentin (an intermediate filament in mesenchymal) and weakly to moderately for S-100 (neural crest cell marker, but expressed in various tumors) and neurone-specific enolase (an enzyme found in neural and neuro-endocrine tissue).2,3,9-10,12 Tumors are rarely positive for glial fibrillary acidic protein (a marker of glial cells), including orbital variants, but several tumors, including meningothelial types, can have multifocal positive reactions for pan-cytokeratin (intermediate filaments in epithelial cells),10,12 although the latter was not seen in the few orbital cases reported to date.3,9-10 The tumors are negative for synaptophysin (a secretory product in neuroendocrine cells).12 One case showed membrane reactivity for E-cadherin (epithelial intercellular junctional protein).6
Treatment for orbital meningiomas usually includes surgical removal of the eye and associated tumor,3,6 although radiation therapy can be applied after surgical removal.13 However, local recurrence is common. In addition, retrobulbar meningiomas can extend intracranially along the optic nerve and can infiltrate the optic chiasm and diencephalon. This can result in blindness in the contralateral eye.3,4,14 Extracranial metastasis is rare but has been reported (e.g. lungs, heart).6,9,14 Median survival times for dogs with retrobulbar meningiomas are not known. In one study with 17 cases in which follow up was available, dogs were still alive for up to 4.5 years after surgical removal alone.3 For dogs with intracranial meningiomas, radiation therapy appears to prolong survival after surgery, with a median survival time of 16.5 months versus 7 months with surgery alone.13
References
- Koestner A, Bilzer T, Fatzer R et al. Histological classification of tumors of the nervous system of domestic animals. Second series, Volume V. Armed Forces Institute of Pathology, Washington, DC. 1999; pp 27-29.
- Higgins RJ, Bollen AW, Dickinson PJ et al. Tumors of the Nervous System. Tumors in Domestic Animals. 5th ed. John Wiley & Sons, Inc.; 2017:834-891
- Mauldin E, Deehr A, Hertzke D et al. Canine orbital meningiomas: a review of 22 cases. Vet Ophthalm 2000;3:11-16.
- Adamo P, Forrest L, Dubielzig R. Canine and Feline Meningiomas: Diagnosis, Treatment, and Prognosis. Comp Contin Educ Pract Vet (North Am edition) 2002;26:951-966.
- Dubielzig R. Tumors of the Eye. In: Meuten D, ed. Tumors in Domestic Animals. 5th ed. John Wiley & Sons, Inc.; 2017:915-916.
- Regan D, Kent M, Mathes R et al. Clinicopathologic findings in a dog with a retrobulbar meningioma. J Vet Diag Invest 2011;23:857-862.
- Cook J, Levine G. Cerebrospinal Fluid and Central Nervous System Cytology. In: Valenciano A, Cowell R, ed. Cowell and Tyler’s Diagnostic Cytology and Hematology of the Dog and Cat. 4th ed. Mosby; 2013:237-238.
- Tvedten H and Hillström A. Cytologic appearance of retinal cells included in a fine-needle aspirate of a meningioma around the optic nerve of a dog. Vet Clin Path 2013;42:234-237.
- Pérez V, Vidal E, González et al. Orbital meningioma with a granular cell component in a dog, with extracranial metastasis. J Comp Pathol 2005;133:212-217.
- Montoliu P, Anor S, Vidal et al. Histologic and immunohistochemical study of 30 cases of meningioma. J Comp Pathol 2006;135:200-207.
- Louis, DN, Scheithauer, BW, Budka, H, et al. Meningiomas. In: Pathology & Genetics: Tumours of the Nervous System, ed. Kleihues, P, Cavenee, WK, 2nd ed., International Agency for Research on Cancer, Lyon, France, 2000; pp. 176–184.
- Barnhart KF, Wojcieszyn J, Storts RW. Immunohistochemical staining patterns of canine meningiomas and correlation with published immunophenotypes. Vet Pathol 2002;39:311-321.
- Axlund T, McGlasson M, Smith A. Surgery alone or in combination with radiation therapy for treatment of intracranial meningiomas in dogs: 31 cases (1989-2002). J Am Vet Med Assoc 2002;221:1597-1600.
- Dugan SJ, Schwarz PD, Roberts SM, et al. Primary optic nerve meningioma and pulmonary metastasis in a dog. J Am Anim Hosp Assoc 1993;29:11–16
Author: Elizabeth Held (intern), edited by Tracy Stokol