
Pleural fluid from a young goat
Case Information
A 9 month old male Billy goat presented to the Cornell Equine & Nemo Farm Animal Medicine Service vocalizing and in respiratory distress. On presentation, the patient was tachycardic (220 beats per minute), vocalizing, and had pale mucous membranes. Point-of-care bloodwork revealed a severe anemia (packed cell volume, 14%), mild to moderate hypoproteinemia (5.8 mg/dL, reference interval (RI): 6.2-8.0 mg/dL), moderate azotemia (blood urea nitrogen 45 mg/dL, RI: 11-27 mg/dL; creatinine 2.1 mg/dL, RI: 0.4-2.2 mg/dL), and a high normal pH with a markedly increased anion gap (29 mmol/L, RI: 5-15 mmol/dL) and evidence of a mixed acid-base disturbance (primary respiratory alkalosis and primary titration metabolic acidosis, with the latter likely due to severe hyperlactatemia [18.6 mmol/L, RI: 0.3-1.5 mmol/L]). A point-of-care CBC revealed a moderate leukocytosis (32.7 x 103/µL, RI: 7.2-17.7 x 103/µL) consisting of a marked neutrophilia (23.5 x 103/µL, RI: 1.9-9.5 x 103/µL) and a moderate monocytosis (2.1 x 103/µL, RI: 0.0-0.9 x 103/µL).
Thoracic ultrasonographic examination was performed, which revealed a left-sided pneumothorax, a moderate amount of free fluid in the cranioventral thorax, and abnormal lung parenchyma. A chest tube was placed in the left side of the thorax and 240mL of air was removed for stabilization purposes. Overnight treatment included flow-by oxygen, intravenous (IV) fluid therapy, and administration of antibiotics and pain medication as well as nebulization with albuterol and N-acetylcysteine.
Repeat blood testing was performed the next day, which still showed a marked anemia (hematocrit 11%, RI: 28-44%) with no evidence of regeneration on smear examination, improving inflammation (segmented neutrophil count 16.0 x 103/µL, RI: 1.9-9.5 x 103/µL, band neutrophil count 0.4 x 103/µL, RI: 0-0.1 x 103/µL, with mild toxic change), mild thrombocytopenia (204 x 103/µL, RI: 247-912 x 103/µL), persistent mild azotemia (urea nitrogen 55 mg/dL, RI: 10-35 mg/dL; creatinine 1.3 mg/dL, RI: 0.3-0.8 mg/dL), and marked hepatocellular injury (AST 2014 U/L, RI: 62-145 U/L; SDH 1700 U/L, RI: 24-63 U/L; GLDH 1150 U/L, No RI) with a mild increase in total and direct bilirubin (total bilirubin 0.3 mg/dL, RI: 0-0.2 mg/dL; direct bilirubin 0.2 mg/dL, RI: 0.0 mg/dL) concentrations. Increased GGT activity (118 U/L, RI: 24-64 U/L) could be attributed to cholestasis, biliary hyperplasia or biliary epithelial necrosis. Total protein and albumin concentrations were decreased (total protein 6.0 g/dL, RI: 6.2-8.0 g/dL; albumin 2.5 g/dL, RI: 2.9-4.0 g/dL), but globulin concentrations were within low normal limits.
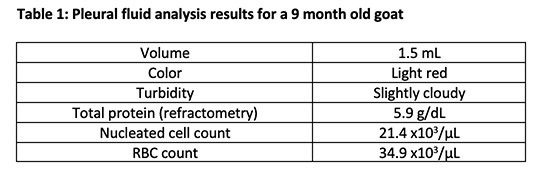
A blood transfusion was administered and a thoracocentesis was performed. The collected pleural fluid was submitted to the clinical pathology laboratory for analysis. Results and images from the pleural fluid analysis are provided below.

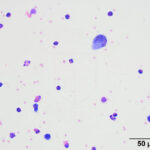
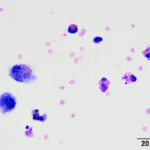
Examine the representative images of the smears or view the digital slide (click on the image to the right) and answer the questions below. Note that the scanned slide is quite thick, so the best area to identify the cells is at the leading edge, which is the thinnest area.
- Considering the predominant leukocyte in the fluid, what is your top differential diagnosis for this patient?
- What other process is occurring based on the appearance of the macrophages in the figures?
|
|
|
Answers on next page