
Laboratory data from an acutely collapsed dog
Case Information
A 1-year-old spayed female Maltese-cross dog was presented as an emergency to Cornell University Hospital for Animals for acute collapse. The dog had been healthy up until this acute event, which happened suddenly during routine play outdoors. On physical examination, the dog was depressed and hypothermic, tachycardic (250 beats per minute) and tachypneic (78 breaths per minute). Systolic blood pressure was low (96 mmHg systolic/68 mmHg diastolic; reported mean ± standard deviation, 120 ± 19 mmHg systolic and 67 ± 14 mmHg diastolic via oscillometric methods1). The dog was painful on abdominal palpation and had profuse bloody diarrhea. A focused assessment with sonography in trauma (FAST) scan of the abdomen revealed a moderate amount of ascites and edema in the mesentery (hyperechoic), gall bladder wall (thickened wall with hyperechoic and hypo-echoic inner and outer walls, respectively), small intestine (diffusely thick and hyperechoic), and pancreas (thicker than normal with anechoic strands). The sonographic results were compatible with edema in multiple organs.
Results of quick assessment tests showed a packed cell volume (PCV) of 52% (reference interval [RI], 42-54%), total solid concentration of 5 g/dL (RI, 5.9-7.8 g/dL), glucose of 359 mg/dL and urea nitrogen of 15-26 mg/dL. A venous blood gas analysis yielded a pH of 7.43 units (RI, 7.32-7.38 units), with a pCO2 of 28 mmHg (RI, 38-46 mmHg), bicarbonate of 18 mmol/L (RI, 20-25 mmol/L) and base excess of -7 mmol/L (RI, -6 to 0 mmol/L). Sodium and chloride concentrations were 149 (RI, 145-151 mEq/L) and 115 (RI, 110-119 mEq/L) mEq/L, respectively. The pO2 was 45 mmHg (RI, 45-67 mmHg). The lactate concentration was 1.7 mmol/L (normal <2.0 mmol/L; measured 15 minutes after the blood gas analysis).
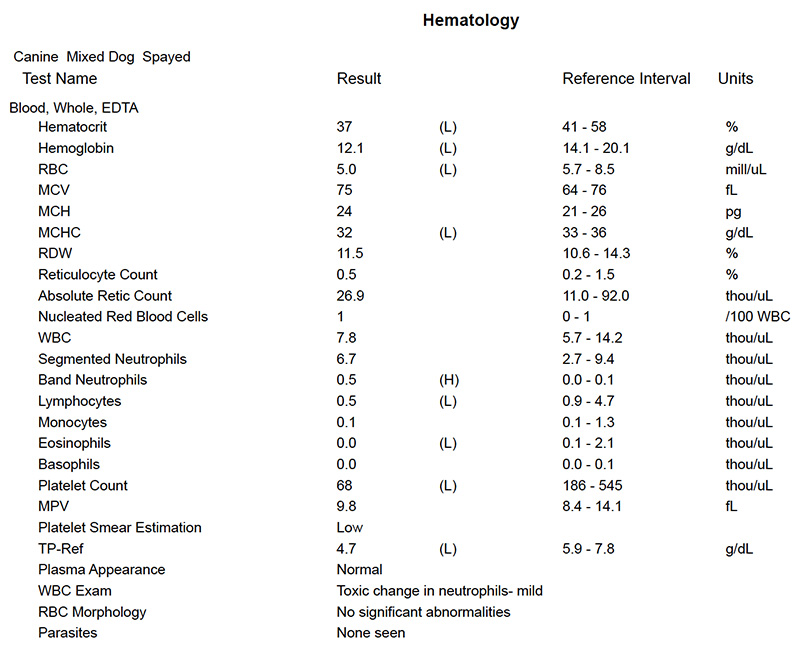
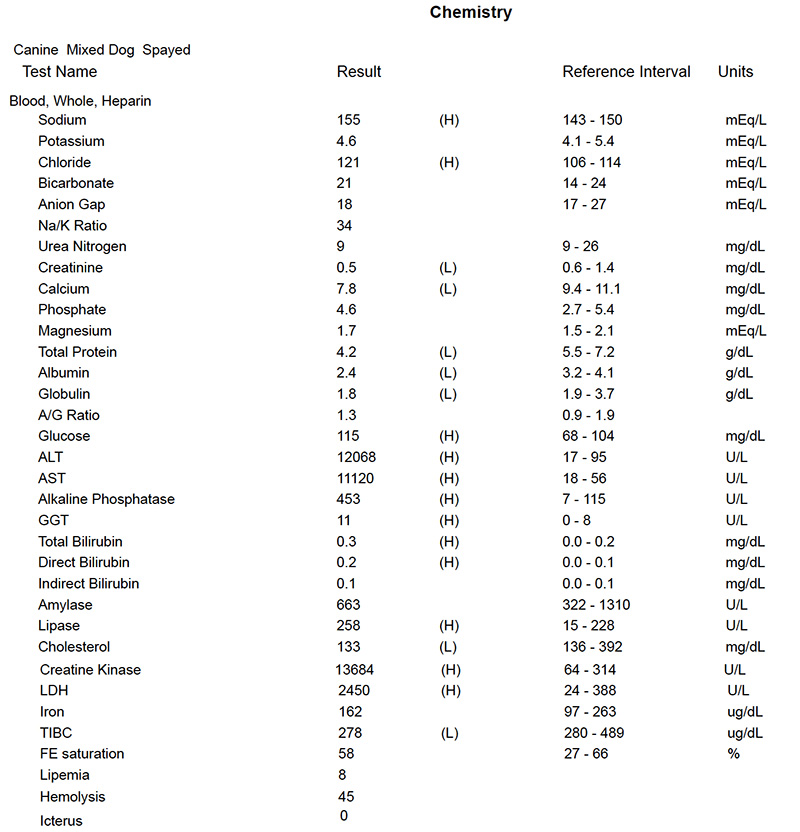
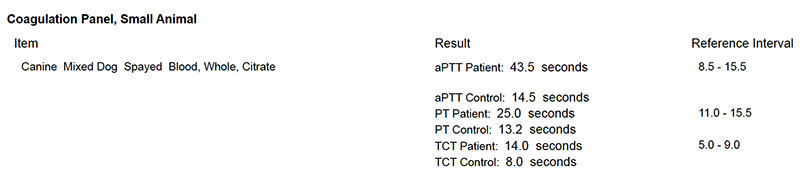
The dog was treated symptomatically with intravenous fluids, anti-emetics, pain relief and antibiotics overnight and blood was taken for a hemogram, coagulation panel, and biochemical profile the next morning. Results are shown below, along with four questions related to the results.
- What is your interpretation of the point-of-care blood gas results?
- Considering the quick assessment tests, how would you interpret the changes in analytes in the hemogram and biochemical profile?
- What pathologic processes are revealed by the clinical pathologic results?
- What is your top differential diagnosis?
Answers on next page