
Pleural fluid from a cat
Case Information
A 13-year-old neutered male Domestic Shorthair was presented to the Cornell University Hospital for Animals for a 2-day history of increased respiratory rate and effort, inappetence, and constipation. The cat was housed indoors and had no known history of trauma. He was diagnosed at a young age with cerebellar hypoplasia and was recently found to be hyperthyroid. On presentation, the cat was weak, had cerebellar ataxia, and was laterally recumbent for the physical examination. Heart sounds were muffled bilaterally and the cat had markedly increased inspiratory effort with abdominal press and tachypnea. He was 5% dehydrated, with diffuse muscle wasting, and a palpable thyroid slip.

A point-of-care venous blood gas analysis revealed acidemia (pH 7.28 units, reference interval [RI]: 7.32-7.42 units) due to a primary hyperchloremic metabolic acidosis (bicarbonate, 16 mmol/L, RI: 20-25 mmol/L; base excess, -10 mmol/L, RI: -4 to 0 mmol/L; disproportionally high chloride versus sodium concentration) with a compensatory respiratory alkalosis (partial pressure of carbon dioxide, 36 mmHg, RI: 38-46 mmHg). There was a mild hyperkalemia (4.8 mEq/L, RI: 3.8-4.5 mEq/L). A fast ultrasonographic scan of the thorax showed a large cavitated mass in the thoracic cavity with a moderate amount of pleural fluid accumulation. Thoracic radiographs revealed severe, bilateral pleural effusion and a moderate to severe, diffuse interstitial to alveolar pulmonary pattern with reduced lung volume and a large caudal thoracic mass (Figure 1). A medium sized, focal, cranioventral abdominal soft tissue mass was also identified along with bilateral, moderate shoulder osteoarthrosis, which was considered an incidental finding (Figure 1). Quick assessment tests revealed a mild anemia (packed cell volume, 24%, RI: 31-48%) and normal total solid concentration of 6.4 mg/dL (RI, 5.9-7.5 g/dL). A triple snap test for feline leukemia virus, feline immunodeficiency virus and heartworm was negative.
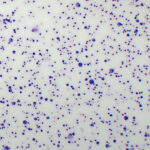
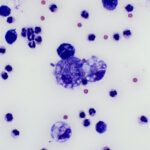
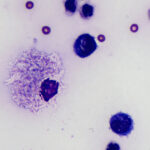
A pleural fluid sample was collected and submitted for cytologic analysis. The fluid was light yellow and opaque with a total protein concentration by refractometer of <2.5 g/dL and a nucleated cell count of 17.5 thou/uL. Examine the representative images of sediment smears of the fluid (Figures 2-4) and answer the questions.
- How would you classify the effusion?
- Is a cause for the effusion evident?
|
|
|
|
Answers on next page