
Interpretation
Metastatic apocrine anal sac adenocarcinoma
Explanation
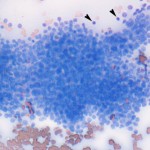
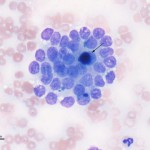
The direct smears of the aspirate contained a moderate amount of blood with numerous packets and clusters of medium sized uniform cuboidal epithelial cells (Figure 1). Several distinct acinar arrangements were seen, which contained blue secretory product (Figure 2). The cells had round to slightly oval eccentric nuclei with lacey chromatin and inapparent nucleoli. They had a moderate amount of pale purple cytoplasm with indistinct boundaries. Anisokaryosis and anisocytosis were mild, however low numbers of individual cells with large nuclei were seen. Mitotic figures were not observed. There were low numbers of lymphocytes in the background. Unfortunately there were too few lymphocytes in the background to confirm aspiration of a lymph node. This was attributed to effacement of the node by the metastatic tumor.
Apocrine anal sac adenocarcinoma has a characteristic cytologic appearance consisting of loosely cohesive clusters of cuboidal cells with a uniform round nuclei and light blue-gray, slightly granular cytoplasm and indistinct cell borders. Cells often have a bland, uniform morphology lacking overt cytologic criteria of malignancy, which does not correlate to the aggressive biologic behavior of the tumor. An acinar arrangement may be one of the features that helps distinguish this neoplasm from a metastatic perianal (hepatoid) carcinoma (the latter neoplasm may also demonstrate pink granules that are typical of hepatoid cells).
|
|
|
Further information and follow-up
A fine needle aspirate of the perianal mass was performed and submitted for cytologic assessment. The submitted smears consisted of several clusters of epithelial cells that corresponded to those seen in the medial iliac lymph node aspirate. Unfortunately, there is no further follow-up information for this case.
Discussion
Apocrine gland adenocarcinoma of the anal sac, also known as anal sac adenocarcinoma, is a malignant tumor arising from the secretory glandular epithelium associated with the wall of the anal sac. It occurs at a relatively low frequency in the dog, representing 17% of perianal tumors and 2% of all “skin” tumors, and is rare in the cat.1 Affected dogs are typically older (median age, 10 years old), however there are reported cases in dogs as young as 5 years of age.2 Historically females were thought to be predisposed to this tumor, but more recent studies report a more equal sex distribution.2,3 In as many as 39% of dogs in one study, anal sac masses were detected as an incidental finding, stressing the importance of a rectal examination as part of a complete physical examination in every adult dog.2 Reported clinical signs include perineal swelling, tenesmus, constipation, diarrhea or change in stool shape, licking or biting at the perineum, perianal bleeding, polyuria/polydipsia,”scooting”, lethargy, and anorexia.2 The tenesmus (as reported in this case) is caused by enlargement of the iliac (also referred to as sublumbar) lymph nodes, which are located ventral to the lumbar spine but dorsal to the rectum. When these lymph nodes are enlarged secondary to metastasis from the primary tumor site, they cause ventral deviation and even partial obstruction of the colon.4 The decreased colonic diameter prohibits passage of a normal sized stool, resulting in compensatory decreased stool size, soft stool, or even diarrhea in some patients. This is also consistent with our case, where the owner reported that the dog had smaller than normal stools. Rarely, regional bone metastasis or direct extension of tumor from the iliac lymph nodes into the lumbar vertebrae with associated pain or fracture may be seen.1
Clinical signs of polyuria and polydipsia with anal sac adenocarcinoma has been attributed to paraneoplastic hypercalcemia, secondary to production of parathyroid hormone-related peptide (PTHrp) by the neoplastic cells.1,4 The incidence of hypercalcemia in anal sac adenocarcinoma ranges from 27-51%, but the corresponding clinical manifestation of polyuria and polydipsia is not always concurrently present.2,3 The hypercalcemia typically resolves with surgical excision of the primary mass and metastatic lymph nodes (if present) and returns with recurrence or metastasis.1,4 The dog in this case was not hypercalcemic and did not display the associated clinical signs.
Anal sac adenocarcinomas are locally invasive and highly metastatic. The tumor usually metastasizes to the regional iliac lymph nodes followed by distant metastasis to the liver, spleen, lungs, and other less common sites.1 Treatment options include surgery (anal sacculectomy with or without lymph node excision), radiation therapy (pre-operative, post-operative, or palliative), and chemotherapy. Reported median survival times of dogs treated with a variety of protocols ranges from 6 to 18 months.2.3 Although one study showed no significant difference in survival comparing surgery alone, radiation therapy alone, surgery with radiation therapy, surgery with chemotherapy, or surgery with chemotherapy and radiation therapy, there was a survival advantage for dogs receiving any type of surgery as a part of their treatment.2 Poor prognostic indicators are primary tumor size, presence of lymph node or distant metastasis, and hypercalcemia, although the assocation of prognosis with hypercalcemia is not a consistent finding across studies.2,3,5
References
- Withrow, S.J. and Vail, D.Ml. Perianal tumors. Small Animal Clinical Oncology: 4th ed. Saunders Elsevier: St. Louis, MO. 2007.
- Williams, L.E. et al. Carcinoma of the apocrine glands of the anal sac in dogs: 113 cases (1985-1995). JAVMA 223: 825-831, 2003.
- Bennett, P.F. et al. Canine Anal Sac Adenocarcinomas: Clinical Presentation and Response to Therapy. J Vet Intern Med 16: 100-104, 2002.
- Gauthier, M. et al. Identifying and treating anal sac adenocarcinoma in dogs. Vet Med Feb 1, 2009.
- Polton, G.A. and M.J. Brearley. Clinical Stage, Therapy, and Prognosis in Canine Anal Sac Gland Carcinoma. J Vet Intern Med 21: 274-280, 2007.