
Interpretation
Mixed inflammation (neutrophils, macrophages) with intralesional keratin
Explanation
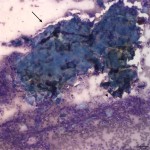
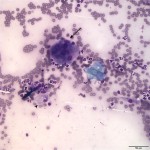
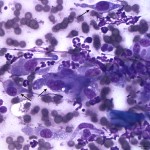
The smear is highly cellular consisting of numerous mixed inflammatory cells and low numbers of mesenchymal cells, often surrounding large amounts of keratinized squamous epithelial cells and keratin debris (Question 1). The inflammatory cells consist mostly of nondegenerate neutrophils with fewer macrophages, including binucleated forms and multinucleated giant cells (Question 1). The mesenchymal cells are fusiform with a centrally placed oval nucleus, and moderate amounts of basophilic cytoplasm that tails off in both directions from the nucleus. These cells are morphologically consistent with fibroblasts (Question 2). Although they do display some cytologic criteria of malignancy (e.g. anisocytosis, anisokaryosis, binucleation), in this setting of marked inflammation these changes are interpreted as reactive (Question 2). Reactive fibroblasts can become quite pleomorphic secondary to inflammation and caution should be exercised when interpreting the presence of pleomorphic mesenchymal cells in the setting of inflammation.
This pattern of inflammation is compatible with a pyogranulomatous or foreign body response. The underlying cause of the inflammation in this case is the keratin (Question 3). The presence of keratin is abnormal in a fine needle aspirate of a tissue lesion because keratinized squamous epithelial cells should not be present under the skin surface. These findings are compatible with the rupture of a follicular cyst or other adnexal skin lesion consisting of keratin, releasing keratin contents into the dermal and subcutaneous tissue (Question 3). Keratin acts an endogenous foreign body, which the body tries to “wall off,” since it is unable to ingest and destroy it. With chronicity, fibroblasts proliferate forming a connective tissue capsule around the inciting agent.
|
|
|
|
Discussion
A cyst is a non-neoplastic, simple sac-like structure with an epithelial lining that determines its classification.1 The majority of skin cysts in dogs and cats are follicular in origin and can be further categorized histologically based on the level of the follicle from which they develop, including: infundibular, isthmus, matrical, and hybrid.1 Infundibular cysts have also been referred to as epidermal cysts, epidermal inclusion cysts, or epidermoid cysts.2-4 The term “sebaceous cyst” is a clinical misnomer and is used due to the nature of the cyst contents when expelled.1 However, sebum is milky white, whereas the keratinaceous contents of follicular cysts are yellow, light brown, or gray material that is semisolid, caseous, granular, or doughy in consistency.1,5
Follicular cysts usually present as solitary, firm nodules ranging from 0.2 to 2cm, with larger lesions of up to 6cm occurring infrequently.1,6 The cysts are present within the dermis, but large cysts can extend into the panniculus (subcutis).4 Follicular cysts can be multiple (disseminated) arising concurrently or progressively over time, however this is relatively uncommon.1,6 A case series reported individual patients having anywhere from an estimated >20 to >200 masses.6 The overlying epidermis is intact with either partial or total alopecia, unless the cyst wall has ruptured or the patient has traumatized the lesion.1 The lesions may appear blue, white, or yellow depending on the depth of the cyst and color of its contents.1
Follicular cysts occur in middle-aged to older dogs and cats.3 Predilection sites include the head, neck, limbs, and dorsum.3,6 Follicular cysts are most frequently associated with continuous blunt trauma or chronic irritation resulting in occlusion of follicular infundibulum and retention of follicle contents (hair and keratin).3 Therefore, they can develop in large breed dogs over pressure points (e.g. elbow), in cats at the site of prior jugular venipuncture, and in surgical scars due to follicular entrapment.3 Reported predisposed breeds for follicular cysts include Boxers, Shih Tzus, Miniature Schnauzers, Old English Sheepdogs, Rottweiler, Doberman Pinschers, and Bullmastiffs.3
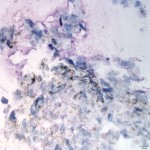
Cytologically, aspirates from intact follicular cysts yield highly cellular samples with large amounts of keratinized squamous epithelial cells and keratin debris, consistent with aspiration of cyst contents (Figure 4).2 Cholesterol crystals are often seen, which represent breakdown of cells within the cyst.2 Fine needle aspiration with cytologic examination is an excellent way to diagnose these lesions.7 Adnexal tumors, such as pilomatricomas and trichoepitheliomas can produce similar cytologic findings, but these are quite rare and usually benign.
The treatment of choice for follicular cysts is surgical excision or monitoring (no treatment).5 Surgical excision is recommended, because these cysts can rupture releasing their keratin contents into the dermis or subcutis inciting a pyogranulomatous inflammatory response, as occurred in this case.3-5 Therefore, cysts should never be squeezed hard or manually evacuated due to the greatly increased chance of expressing cyst contents into deep tissues, thus inciting inflammation.5 Ruptured follicular cysts can result in pain and pruritus leading to the patient self-traumatizing the area with potential subsequent secondary bacterial infection.5,6 With disseminated follicular cysts where surgical excision may be impractical, treatment with high dose isotretinoin may be worthwhile. This drug has been shown to result in no new cyst formation in a dog, however it did not result in resolution of pre-existing cysts.6
References
- Gross TL, Ihrke PJ, Walder EJ, Affolter VK. Skin Diseases of the Dog and Cat: Clinical and Histopathologic Diagnosis. 2nd ed. Oxford, UK: Blackwell Science Ltd, 2005. 607-612.
- Raskin RE, Meyer DJ. Canine and Feline Cytology: A Color Atlas and Interpretation Guide. 2nd ed. St.Louis, MO: Saunders Elsevier, 2010. 26-28.
- Goldschmidt MH, Shofer FS. Skin Tumors of the Dog and Cat. Oxford, UK: Pergamon Press, 1992. 271-279.
- Goldschmidt MH, Dunstan RW, Stannard AA, et al. Histologic classification of epithelial and melanocytic tumors of the skin of domestic animals. Second series, Vol III. Washington, DC: Armed Institute of Pathology, 1998. 33.
- Miller WH, Griffin CE, Campbell KL. Muller & Kirk’s Small Animal Dermatology. 7th ed. St. Louis, MO: Elsevier, 2013. 825-826.
- White A, Stern A, Campbell K, Santoro D. Multiple (disseminated) follicular cysts in five dogs and one cat.2013 Sep 21. Vet Rec. 173 (11). 269-271.
- Ghisleni G, Roccabianca P, Ceruti R, et al. Correlation between fine-needle aspiration cytology and histopathology in the evaluation of cutaneous and subcutaneous masses from dogs and cats. 2006. Vet Clin Pathol. 35 (1). 24-30.
Authored by: Drs. Newman (clinical pathology resident) and T. Stokol.