
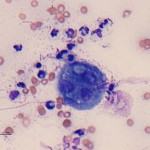
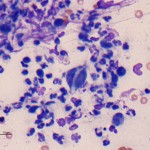
Photomicrographs of a fine needle aspirate from a femur mass in a dog
Case information
A 6 year old spayed female Labrador Retriever presented with a 2 month history of intermittent left hind limb lameness and a one day history of edema in that limb. Treatment with non-steroidal anti-inflammatory and pain-relieving drugs resulted in some improvement initially, but the lameness had returned and was more severe. On presentation, the dog avoided bearing weight on the left hind limb, which was swollen and erythematous. A firm and large right prescapular lymph node was palpated and the left inguinal and popliteal lymph nodes were also enlarged. Rectal examination revealed enlarged inguinal lymph nodes. Heart and respiratory rates were normal and the dog was not febrile. A hemogram revealed a mild leukocytosis (15.2 x 103/uL, reference interval, 5.7-14.2 x 103/uL), due to a mild neutrophilia (11.4 x 103/uL, reference interval, 2.7-9.4 x 103/uL) and a mild monocytosis (1.7 x 103/uL, reference interval, 0.1-1.3 x 103/uL). A serum biochemical panel revealed a mild hypoalbuminemia (2.7 g/dL, reference interval, 3.1-4.2 g/dL), a mild hyperglobulinemia (3.7 g/dL, reference interval, 1.9-3.6 g/dL), mildly decreased serum iron (76 ug/dL, reference interval, 78-261 ug/dL), and mildly decreased total iron binding capacity (240 ug/dL, reference interval, 270-496 ug/dL). No abnormalities were detected in a urinalysis. Radiographic examination revealed an aggressive bone lesion with a periosteal reaction in the proximal left femur. Thoracic radiographs revealed possible lymphadenopathy. Ultrasonographic examination of the left hind limb revealed a hypoechoic mass surrounding the bone with an irregular periosteal reaction. Multifocal lymphadenopathy (bilateral medial iliac, hypogastric and sacral lymph nodes) was observed on ultrasonographic examination of the abdomen. A fine needle aspirate was performed on the left femur mass.
Evaluate the representative photomicrographs below and consider the following questions:
- What cell types are present in the aspirate and do they indicate inflammation (if so, what type) or neoplasia?
- Is a cause for the mass lesion evident in the aspirate?
- Do these findings explain the hematologic and serum biochemical results?
|
|
|
Answer on next page