
Interpretation
Hepatocellular carcinoma
Explanation
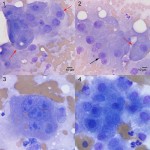
The cells in the aspirate were observed in flat sheets and small clusters, with some individualization. They were cuboidal to polygonal and had low to moderate nuclear to cytoplasmic ratios and a grainy pink cytoplasm with distinct boundaries. They resembled hepatocytes but displayed numerous criteria of malignancy, including marked anisocytosis and anisokaryosis, maronucleoli, multiple nucleoli and pronounced multinucleation. There was no evidence of inflammation or an infiltrative neoplasm (such as systemic spread of the previously diagnosed and current mast cell tumors).
|
|
Discussion
Hepatocelluar carcinomas have a relatively low incidence rate in dogs (they account for less than 1% of all canine neoplasms) and are more frequent in male dogs.1 Hepatocellular carcinomas pose a diagnostic challenge because they can appear cytologically normal and have a diffuse distribution in the liver. Hepatocellular carcinomas must be differentiated from regenerative/hyperplastic lesions and adenomas. Size can occasionally be used to help rank these differential diagnoses, because most nodular hyperplastic lesions are reported to be 3 cm or less in diameter. However, adenomas can be much larger and typically range from 2 to 8 cm in diameter. Histopathologic assessment of lobular architecture, associated fibrosis, and depth of hepatic plates are essential in differentiating these processes.2 Cytologic evaluation is typically more sensitive in detecting inflammation and infiltrative neoplastic processes in the liver than primary hepatocellular tumors.3 In this particular case, the prominent features of malignancy in the majority of hepatocytes from this animal’s liver mass coupled with the lack of any infiltrative population and the clinical description of the mass made a cytological diagnosis possible. The biochemical evidence of liver injury (increased ALT and AST) is a common finding in hepatocellular carcinomas, but is not specific for a neoplastic process. Hepatocellular carcinomas have been reported to cause paraneoplastic hypoglycemia by producing insulin-like growth factor II.4 Hyperalbuminemia has also been documented as a paraneoplastic syndrome in canine hepatocellular carcinoma, likely through excessive synthesis of this protein.5 However, we cannot confirm that these biochemical abnormalities were a paraneoplastic event in this dog because additional serum chemistry panels were not performed (to confirm resolution subsequent to tumor removal) and other causes were not definitively ruled out. Neoplastic hepatocytes have also been reported to produce α-fetoprotein, which may serve a serum tumor biomarker. Unfortunately, not all hepatocellular tumors produce this protein and increased serum α-fetoprotein has also been reported in inflammatory liver diseases.6 Surgical removal is considered the standard treatment for hepatocellular carcinomas, with treated dogs having a median survival time of > 1,460 days compared with 270 days in untreated dogs.7 Studies evaluating the effectiveness of combining resection with chemotherapy, such as gemcitabine,8 have not demonstrated any improvement in clinical outcomes.
Follow up
The dog went to surgery and the mass was successfully removed and submitted for histopathology, which confirmed the cytologic diagnosis. The animal was discharged and returned a few months later with clinical signs of lethargy, inappetance and a painful abdomen. Upon diagnostic evaluation, diffuse masses were found throughout the animal’s liver and a large splenic mass was also discovered. The owners elected humane euthanasia and private cremation.
References
- Meuten DJ. Tumors of the Liver and Gall Bladder. In: Tumors in Domestic Animals, 4th ed. Blackwell Publishing. 2002; pp 483-497.
- Roth L. Comparison of Liver Cytology and Biopsy Diagnoses in Dogs and Cats: 56 Cases. 2001; Vet Clin Pathol, 30(1): 35-38.
- Weiss D. Blauvelt M, Aird B. Cytologic Evaluation of Inflammation in Canine Liver Aspirates. 2001; Vet Clin Pathol, 30(4): 193-196.
- Zini E, Glaus TM, Minuto F, Arvigo M, Hauser B, Reusch CE. Paraneoplastic hypoglycemia due to an insulin-like growth factor type-II secreting hepatocellular carcinoma in a dog. 2007; J Vet Intern Med, 21(1):193-5.
- Cooper ES, Wellman ML, Carsillo ME. Hyperalbuminemia associated with hepatocellular carcinoma in a dog. 2009; Vet Clin Pathol, 38(4):516-20.
- Kitao S, Yamada T, Ishikawa T, Madarame H, Furuichi M, Neo S, Tsuchiya R, Kobayashi K. Alpha-fetoprotein in serum and tumor tissues in dogs with hepatocellular carcinoma. 2006; J Vet Diagn Invest, 18(3):291-5.
- Liptak JM, Dernell WS, Monnet E, Powers BE, Bachand AM, Kenney JG, Withrow SJ. Massive hepatocellular carcinoma in dogs: 48 cases (1992-2002). 2004; J Am Vet Med Assoc, 225(8):1225-30.
- Elpiner AK, Brodsky EM, Hazzah TN, Post GS. Single-agent gemcitabine chemotherapy in dogs with hepatocellular carcinomas. 2011; Vet Comp Oncol, 9(4):260-85.