
Interpretation
Multiple myeloma
Explanation
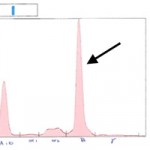
Rouleaux formation is due to is due to charge interactions between RBC membranes and plasma macromolecules and is seen as RBCs forming linear rows like stacks of coins. Rouleaux is often present in the deeper, denser areas of the blood smear but it is considered abnormal when it extends close to the feathered edge. Increased rouleaux formation is often due to an increase in plasma macromolecules, specifically globulins (Question 1).1 The increase in globulins is confirmed on the chemistry panel in this case. The bone marrow aspiration was indicated given the presence of a bicytopenia on the CBC (non-regenerative anemia and neutropenia). Bone marrow cellularity was markedly increased attributable to large numbers of plasma cells (Question 2). The plasma cells are relatively well-differentiated with eccentric nuclei, deep blue cytoplasm and a perinuclear clear zone; they represent approximately 50% of the marrow cellularity with focal areas having close to 80% plasma cells. The finding of over 20% plasma cells in the bone marrow is suggestive of multiple myeloma, which is a neoplastic proliferation of plasma cells that invades the bone marrow. The neoplastic plasma cells usually produce an overabundance of one type (or clone) of immunoglobulin resulting in a hyperglobulinemia (as seen above) and a monoclonal gammopathy.2 Further testing in the form of serum protein electrophoresis (Question 3) is needed to confirm that the hyperglobulinemia is due to an increase in one type of immunoglobulin (monoclonal gammopathy) as opposed to several different globulin types (polyclonal gammopathy). This was done and is shown in Figure 3a (note the electrophoresis from a normal dog in Figure 3b). The patient’s electrophoretogram shows a sharp peak in the beta region corresponding to a monoclonal gammopathy. These findings confirm the diagnosis of multiple myeloma. This diagnosis does explain the ocular signs for which this dog initially presented for (Question 4). Ocular signs associated with multiple myeloma include anterior uveitis, glaucoma, retinal hemorrhages and retinal detachment. It has been reported that 35% of dogs with multiple myeloma have ocular disease3 and occasionally ocular signs are the main presenting complaint.4 The non-regenerative anemia, neutropenia and increased ionized calcium are also a result of the tumor and infiltration of the bone marrow by the neoplastic plasma cells.
|
|
|

Discussion
Multiple myeloma represents approximately 8% of hematopoietic tumors in dogs and is usually seen in older dogs (average age of 8-9 years).3 In most cases of multiple myeloma the neoplastic plasma cells produce large amounts of a single type of immunoglobulin (either IgG, IgA or IgM). Hyperviscosity of the blood occurs if the immunoglobin molecules are large or if they polymerize (usually with IgM or IgA classes).2,3 This single class of immunoglobulin is evident on protein electrophoresis as a single sharp peak either in the beta or gamma region of the tracing (as seen in Figure 3a), though further testing is needed to identify the specific class of immunoglobulin produced. The clinical signs of multiple myeloma result from infiltration of the bone marrow and other organs by neoplastic plasma cells and from increases in immunoglobulins. The most common of the clinical signs associated with this disease are vague consisting of lethargy and weakness, seen in 62% of cases in one study.3 Other findings include radiographic evidence of osteolysis from tumor production of osteoclast-activating factor which is often accompanied by lameness and hypercalcemia.2 Bleeding tendencies, usually epistaxis and gingival bleeding, are also common due to a variety of mechanisms which decrease platelet function and the patient’s ability of clot. Renal lesions may also occur secondary to plasma cell infiltration of the kidneys, renal damage from hypercalcemia and/or filtration of immunoglobulin light chains (or Bence Jones proteins) which may result in polyuria and polydipsia.2 Ocular abnormalities are seen frequently, often secondary to hyperviscosity which results in increased vascular volume and hemorrhage. Ocular lesions include retinal hemorrhage, retinal detachment, anterior uveitis and secondary glaucoma.3,4
The diagnosis of multiple myeloma is made based on finding at least two of the following four criteria:5
- Bone marrow plasmacytosis: greater than 20% plasma cell in a bone marrow aspirate.
- Lytic bone lesions, often seen in the lumbar spine and pelvis.
- Monoclonal gammopathy in serum.
- Bence Jones protein in the urine.
A definitive diagnosis was made in the current case by demonstrating 1. and 3.
Further information and follow up
Following diagnosis, the patient was treated with chemotherapy consisting of melphalan combined with prednisone. This chemotherapy protocol has a greater than 90% response rate in dogs, though long term prognosis is still guarded with a median survival time of 1.5 years. Dogs with hypercalcemia, bleeding tendencies or extensive bony lysis have a poorer prognosis.3 The patient was also treated with tramadol for pain management and topical antibiotic drops for the right eye. Over a course of three months of therapy globulin levels have steadily declined but are still mildly elevated (4.3 g/dL; ref. 1.9-3.6) and other than a very mild anemia (Hct=40; ref. 41-58), hematologic parameters have normalized. The corneal lesions affecting the right eye have healed but this eye is now functionally blind. On last recheck, his owner’s report that he doing very well at home with normal activity level and appetite and no signs of pain. The patient will continue to be monitored through repeat CBC and chemistry panels. Serial electrophoresis can also be used to monitor response to treatment.
References
- Stockham SL, Scott MA. Erythrocytes. In: Stockham SL, Scott MA, eds. Fundamentals of Veterinary Clinical Pathology. 2nd ed. Ames, IO: Blackwell Publishing, 2008;136.
- Vail DM. Plasma Cell Neoplasms. In: Withrow SJ, Vail DM, eds. Small Animal Clinical Oncology. 4th ed. St. Louis, MO: Saunders Elsevier, 2007;769-84.
- Matus RE, Leifer CE, MacEwen G, et al. Prognostic factors for multiple myeloma in the dog. JAVMA 1986;188(11):1288-92.
- Hendrix DVH, Gelatt KN, Smith PJ, et al. Opthalmic disease as the presenting complaint in five dogs with multiple myeloma. J Am Anim Hosp Assoc 1998;34:121-8.
- MacEwen EG, Hurvitz AI. Diagnosis and management of monoclonal gammopathies. Vet Clin N Am Sm Anim Pract 1977;7:119-32.