
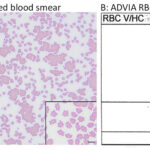
Venous blood smear and RBC cytogram from a cat
Case Information
A 17 year old castrated male Domestic Long Hair cat was presented on a weekend to the Cornell University Hospital for Animals Emergency Service for a suspected gastric foreign body diagnosed with abdominal radiography by the referring veterinarian. The cat had a history of chronic kidney disease, which was being managed with a calcium channel blocker (amlodipine) and a renal diet. On physical examination, the cat was quiet and alert with a body condition score of 3/9, pink and tacky mucous membranes, and an estimated 6% dehydration. The cat had a grade 4/6 left parasternal heart murmur with strong regular pulses. Point-of-care bloodwork revealed a blood urea nitrogen concentration of 50-80 mg/dL as measured with an azostix and a packed cell volume of 33%. The cat also had a metabolic acidosis with respiratory compensation and hyperlactemia. The cat was admitted and treated overnight with amlodipine, intravenous fluids, and an anti-emetic (maropitant). An ultrasonographic examination revealed a foreign body in the stomach and bilaterally small kidneys. Surgery was delayed until the cat was rehydrated and stable.
Prior to surgery (48 hours after admission), blood was drawn into vacutainer tubes containing EDTA or no anticoagulant (Becton Dickinson and Co., Franklin Lakes, NJ, USA) for a screening complete blood profile (CBC) (ADVIA® 2120i) and serum biochemical panel (Cobas 501), respectively. The CBC revealed a moderate non-regenerative anemia (hematocrit: 19%, reference interval [RI]: 31-48%; hemoglobin concentration: 6.8 g/dL, RI: 10.9-15.7 g/dL; absolute reticulocyte count: 13.9 thou/μL, RI: 8.5-60.7 thou/μL). Serum biochemical testing showed mild increases in creatinine concentration (2.4 mg/dL, RI: 0.8-2.1 mg/dL) and aspartate aminotransferase (AST, 71 U/L, RI: 17-48 U/L) and creatine kinase (CK, 1951 U/L, RI: 47-386 U/L) activities. View the provided image of the blood smear and RBC cytogram from the hematology analyzer and answer the questions below:
- What abnormality is present on the smear and the cytogram plot?
- What is the diagnostic relevance of the abnormality?
- What would you do next to confirm that the abnormality is a pathologic finding?
|
|
Answers on next page