
Interpretation
Septic suppurative inflammation with presumptive Campylobacter infection
Explanation
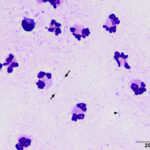
Direct smears of the aspirate were highly cellular and contained many non-degenerate neutrophils (Figures 1 and 2). Numerous bacteria were seen in the background and were slender with wavy to spiral to seagull-like shapes, features typical of Campylobacter (Question 2). Bacteria were not identified intracellularly. No hepatocytes were seen. Results were consistent with a hepatic abscess, as suspected from the imaging findings (Question 1). Since Campylobacter species (sp.) can be part of the normal intestinal flora,1-4 an ascending infection from the biliary system was suspected. Aspiration of adjacent areas of the liver was recommended to rule out an underlying tumor, but was not performed, likely due to the thin rim of tissue surrounding the cystic mass.
|
|
|

Follow up
After the ultrasonographic examination, the dog became hypotensive, which did not respond to intravenous fluid supplementation. The dog was stabilized with vasopressors and an abdominal laparotomy was performed. The surgery revealed a large cystic mass in the left lateral liver lobe and irregular nodules in the left medial and quadrate liver lobes. The left lateral lobe was resected and the remaining two lobes were biopsied. The liver tissue was placed in 10% formalin and submitted for histologic evaluation. A section of the left lateral liver lobe was submitted for aerobic and anaerobic culture. No organisms grew on aerobic culture, but a small growth of Campylobacter sp. was observed after extended anaerobic culture and was speciated as Campylobacter jejuni with mass spectrophotometric analysis (MALDI-TOF).
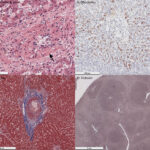
On histologic examination, the left lateral liver lobe contained a well-circumscribed, multiloculated cystic mass, composed of cords and trabeculae of uniform cuboidal epithelial cells, supported by a variably thick fibrous stroma, containing blood vessels. There were large areas of necrosis and the dilated or cystic regions of the mass contained neutrophils, fibrin, degrading cells, and erythrocytes (Figure 3A-C). The sections of the left medial and quadrate liver lobes showed scattered multifocal areas of necrotic hepatocytes, fibrosis surrounding biliary profiles and indistinct nodules (presumably regenerative) (Figure 3D). Hepatocytes contained moderate amounts of red-brown cytoplasmic pigment, compatible with copper; this finding was most evident in zone 1 (periportal) but extended into other zones (Figure 4A, B). The peribiliary fibrosis was confirmed with a trichrome stain and a reticulin stain highlighted the hepatic nodules (Figure 4C, D). The histologic diagnosis was a biliary hamartoma (also known as von Meyenburg complex, left lateral lobe) with random multifocal acute necrotizing hepatitis, peribiliary fibrosis and copper accumulation (grade 3 of 5) (left medial and quadrate lobes).
|
|
|

Follow up
After surgery, the dog had delayed recovery and was found to be hypothermic. Point-of-care blood testing showed a severe acidemia (pH 7.12 units, RI, 7.32-7.38 units) due to a mixed primary respiratory acidosis (pCO2 54 mmHg, RI, 38-46 mmHg) and metabolic acidosis (bicarbonate concentration 17 mmol/L, RI, 20-25 mmol/L; base excess -12 mmol/L, RI, -4 to 0 mmol/L). The strong ion difference was still within reference intervals at 38.3 mEq/L. There was a concurrent hypokalemia (3.3 mEq/L, RI, 3.9-5.1 mEq/L), free ionized hypocalcemia (1.15 mEq/L, RI, 1.18-1.37 mEq/L) and ongoing hyperlactatemia (2.8 mmol/L, normal <2 mmol/L). The hypoglycemia had resolved but monitoring of urine output revealed oliguria. Due to the poor prognosis, the owners elected euthanasia.
Discussion
Campylobacter (C.) sp. are microaerophilic motile slender gram-negative rods that are normal constituents of the gastrointestinal flora of mammals and birds.1–4 They are considered one of several enteropathogenic bacteria, being associated with gastroenteritis in dogs and human beings.2–4 Of the different Campylobacter sp, C. jejuni is the most common form associated with gastroenteritis,2,3 with the other species being of unclear pathogenicity in dogs.4 Campylobacteriosis is a zoonotic disease, however the organism appears to be more frequently sourced from contaminated water or food versus fecal shedding of pets.2–4 Indeed, C. jejuni is considered the most common bacterial cause of food-associated disease in human beings, particularly in industrialized countries.5
Extraintestinal infections in the liver and other organs, such as the pancreas, are rare complications of Campylobacter infections in human beings, dogs, captive monkeys and horses. Several Campylobacter sp. have been detected in the liver of human beings or animals with hepatitis, hepatic cysts or hepatic abscesses, including C. jejuni, as found in the dog of this report.6–11 The bacteria are thought to reach the liver via the biliary system, portal vein or arterial supply from bacteremia, although translocation across the intestinal wall has also been proposed as an alternative route of hepatic infection.7 The motile nature of the organism, which typically contains a flagellum at one or both poles,3 is thought to contribute to its pathogenicity,5 allowing it to invade into intestinal epithelial cells or the biliary system, and potentially through the intestinal wall. Considering the history of diarrhea in the case herein, the organism was thought to have ascended via the bile duct on initial cytologic analysis. However, the cause of diarrhea in the dog was not ascertained (it could have been unrelated to Campylobacter, which is only one of several enteropathogenic bacteria4) and the dog had clinical signs and laboratory test results compatible with systemic sepsis. Thus, an alternative route of infection could have been hematogenous from a bacteremia, particularly given that the underlying abscessed lesion was a biliary hamartoma (which does not connect to the biliary tree). The organism does proliferate readily in bile,12 which may explain liver infections in animals and human beings and the presence of bacteria within bile ducts in histologic sections.6 Underlying immune compromise is thought to predispose human beings3,8 and animals to extraintestinal Campylobacter infections, including simian immunodeficiency virus infection in Macaques6 and chronic oclacitinib therapy in a dog with a hepatic abscess.7 However in our and other reported cases,10,11 there was no obvious cause of immunosuppression.
In the case herein, the bacteria were readily observed extracellularly in direct smears of an aspirate of the cystic liver mass. In another dog with a hepatic abscess, the organism was detected in low numbers extracellularly and phagocytized within neutrophils in an aspirate of the abscess but not in smears of adjacent liver parenchyma or peritoneal fluid.7 In the case herein and the previous report, the organisms were identified as likely Campylobacter sp. based on their characteristic spiral, curved or seagull-like shape. However, the authors of a consensus statement on enteropathogenic bacteria cautioned against the definitive identification of Campylobacter sp. by shape alone in cytologic specimens, because other bacteria, such as Arcobacter, can have curved shapes and these bacteria, as well as certain species or subspecies of Campylobacter, are not considered pathogenic. They recommended speciation via molecular testing since culture alone is not definitive.4 In fact, the organism can be difficult to grow in culture, requiring anaerobic or microaerophilic conditions, different temperatures (including 37 and 42°C; the organism is considered thermotolerant) or culture media, and prolonged culture conditions.3,7–10 Thus, in cases with suspected bacterial infection (e.g. necrotizing or suppurative hepatitis or abscessation), molecular testing may be required to confirm an infection.8 In the dog herein, the organism was cultured after several days in anaerobic conditions and was speciated by MALDI-TOF. In our case and other reported cases, bacteria were not identified in histologic specimens, even when additional stains, including immunohistochemistry for bacterial antigens or silver or gram stains were performed.7,11 In another report, bacteria were present in H&E-stained histologic sections and could be highlighted by silver stains.6 Neither a silver or gram stain were applied to the histologic sections from this dog’s liver.
Hepatic abscesses are an uncommon finding in dogs. In most cases, bacteria other than Campylobacter sp. are cultured from the lesion, including Escherichia coli, Clostridium sp., Klebsiella sp. and various cocci.13–15 However, it is possible that infections with Campylobacter sp. are underdiagnosed due to the fastidious nature of the bacteria and difficult in verifying its presence via culture. The cause of hepatic abscessation in dogs is unknown, but trauma, parasitic infection, bacteremia, and ascending biliary infections have been posited theories. Hepatic abscesses in an older dog should raise consideration for underlying neoplasia, such as a hepatocellular carcinoma, as seen in a previous report of a dog with a hepatic abscess and Campylobacter infection7 and in 21-30% of dogs in two case series of hepatic abscesses.14,15 In this case, the underlying lesion that was abscessed was a biliary hamartoma or von Meyenburg complex.
A biliary or bile duct hamartoma is a congenital malformation of the ductal plate (embryonic precursor of bile ducts), which results in a benign proliferation of uniform biliary epithelial cells supported by fibrous stroma of varying thickenss. The lesion is thought to be initiated from failure of involution of small interlobular embryonic bile ducts. In human beings, the lesions are typically small (average size of 1 cm or less), typically located in subcapsular or periportal lesions and are frequently multiple and found diffusely throughout the liver or confined to one liver lobe.16,17 The lesions are often cystic and may contain bile within cystic regions, but are not connected to the biliary system. They are usually incidental findings in older adults but have been rarely associated with malignant transformation to intrahepatic cholangiocarcinoma. The main issue is that they prompt extensive diagnostic testing for underlying neoplasia because they can mimic hepatic tumors on imaging studies.16,17 There are rare individual case reports in companion animals, including a dog with a single polycystic mass and a cat with multiple lesions, some of which formed a large mass.18,19 In the dog, the epithelial cells were positive for cytokeratin-19 on immunostaining,19 supporting a biliary origin.20 Differential diagnoses include biliary cystadenoma, cystic lesions in the liver such as polycystic liver disease, or fibroadenoma. Other authors have used the presence of multiple lesions in tissue adjacent to a main mass18 or absence of mitotic figures in the stromal cells19 as evidence for a hamartoma over a cystadenoma or fibroadenoma, respectively. One could argue that the formation of a large mass would favor a diagnosis of a biliary cystadenoma, however the distinction between this tumor and a hamartoma is of little clinical relevance, because they are both benign lesions. Inflammation or abscessation has not been reported to be a prominent component of biliary hamartomas, as we saw in our case. However, recurrent sepsis in a human patient was attributed to sequestration of bacteria (E. coli and Klebsiella) in underlying hamartomas in a single case report, despite no other evidence for bacteria within the lesion.21
Author: T. Stokol
Acknowledgements: Dr. Demeter performed the histological analysis in this case.
References
- Suchodolski JS. Companion animals symposium: microbes and gastrointestinal health of dogs and cats. J Anim Sci. 2011 May;89(5):1520–30.
- Iannino F, Salucci S, Di Donato G, Badagliacca P, Vincifori G, Di Giannatale E. Campylobacter and antimicrobial resistance in dogs and humans: “One health” in practice. Vet Ital. 2019 Sept 30;55(3):203–20.
- Facciolà A, Riso R, Avventuroso E, Visalli G, Delia SA, Laganà P. Campylobacter: from microbiology to prevention. J Prev Med Hyg. 2017 June;58(2):E79–92.
- Marks SL, Rankin SC, Byrne BA, Weese JS. Enteropathogenic bacteria in dogs and cats: diagnosis, epidemiology, treatment, and control. J Vet Intern Med. 2011 Nov;25:1195–208.
- Dasti JI, Tareen AM, Lugert R, Zautner AE, Gross U. Campylobacter jejuni: a brief overview on pathogenicity-associated factors and disease-mediating mechanisms. Int J Med Microbiol. 2010 Apr;300(4):205–11.
- Clemmons EA, Jean SM, Machiah DK, Breding E, Sharma P. Extraintestinal campylobacteriosis in rhesus macaques (Macaca mulatta). Comp Med. 2014 Dec;64(6):496–500.
- Boston TA, Lawhon SD, Aitee GF, Como K, Sannajust K, Gremillion CL, et al. Isolation of Campylobacter upsaliensis From an Abscessed Hepatic Mass in a Dog. J Vet Intern Med. 2025 Aug 14;39(5):e70195.
- Han XY, Tarrand JJ, Rice DC. Oral Campylobacter species involved in extraoral abscess: a report of three cases. J Clin Microbiol. 2005 May;43(5):2513–5.
- Ohkoshi Y, Sato T, Murabayashi H, Sakai K, Takakuwa Y, Fukushima Y, et al. Campylobacter upsaliensis isolated from a giant hepatic cyst. J Infect Chemother. 2020 July;26(7):752–5.
- Wetsch NM, Somani K, Tyrrell GJ, Gebhart C, Bailey RJ, Taylor DE. Campylobacter curvus-associated hepatic abscesses: a case report. J Clin Microbiol. 2006 May;44(5):1909–11.
- Macías-Rioseco M, Ochoa J, Choi EA, Blanchard P, Moeller RB, Uzal FA. Campylobacter jejuni hepatitis in a horse: case report and literature review. J Vet Diagn Invest. 2025 May;37(3):463–6.
- Blaser MJ, Hardesty HL, Powers B, Wang WL. Survival of Campylobacter fetus subsp. jejuni in biological milieus. J Clin Microbiol. 1980 Apr;11(4):309–13.
- Farrar ET, Washabau RJ, Saunders HM. Hepatic abscesses in dogs: 14 cases (1982-1994). J Am Vet Med Assoc. 1996;208:243–7.
- Burke JE, Hess RS, McEntee EP, Griffin MA, Harmon SM, Silverstein DC. Hepatic abscessation in dogs: A multicenter study of 56 cases (2010-2019). J Vet Emerg Crit Care (San Antonio). 2023;33(6):665–75.
- Dickerson V, Poses B, Hyndman P, McPhetridge J, Scharf V, Matz B, et al. Outcome in 38 dogs surgically treated for hepatic abscessation. Vet Surg. 2023 Jan;52(1):127–33.
- Sheikh AAE, Nguyen AP, Leyba K, Javed N, Shah S, Deradke A, et al. Biliary Duct Hamartomas: A Systematic Review. Cureus. 14(5):e25361.
- Pech L, Favelier S, Falcoz MT, Loffroy R, Krause D, Cercueil JP. Imaging of Von Meyenburg complexes. Diagn Interv Imaging. 2016 Apr;97(4):401–9.
- Naghi R, Bertran J, Spoldi E, Dark MJ, de Oliveira HH, Souza C, et al. Multiple biliary duct hamartomas in a cat resulting in a hepatic mass: A case report. Vet Med Sci. 2023 June 29;9(4):1441–5.
- Mao D, Song X, Ma D, Hu S, Zhang Z, Wang J, et al. Bile duct hamartoma in a dog. J Comp Pathol. 2023 Nov;207:45–9.
- Pillai S, Center SA, McDonough SP, Demarco J, Pintar J, Henderson AK, et al. Ductal Plate Malformation in the Liver of Boxer Dogs: Clinical and Histological Features. Vet Pathol. 2016 May;53(3):602–13.
- Santos MB, Ponta Garça M, Vieira B, Ávila P, Freitas A. Recurrent sepsis in a patient with biliary hamartomas. Eur J Case Rep Intern Med. 2023 Mar 10;10(3):003764.