
Biochemical results from a vomiting dog
Case information:
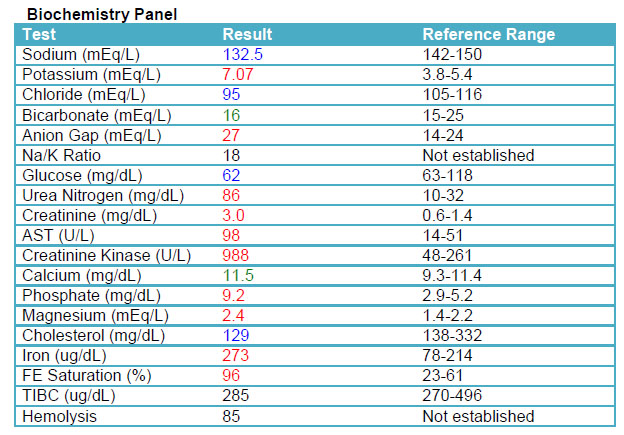
A 2 year-old male castrated Cane Corso presented to the Cornell University Hospital for Animals for a two-day history of vomiting, hypoglycemia, and bradycardia. Blood-work performed at the referring veterinarian revealed a hyponatremia and hyperkalemia. No abnormalities were found on abdominal radiographs. Prior to referring the dog to the Cornell Emergency service, the rDVM began treatment with a bolus of 50% dextrose and 0.9% NaCl. The dog had a previous history of hospitalization for sepsis, vomiting, and diarrhea that had occurred one week after vaccination for rabies and distemper. Consequently, all vaccine protocols were discontinued and were therefore not up-to-date.
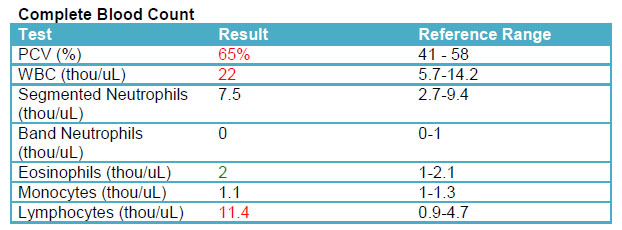
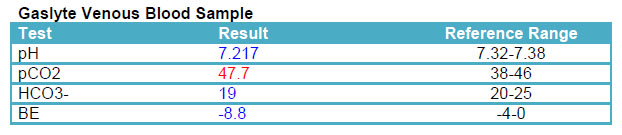
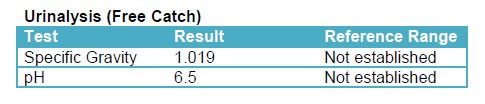
On presentation, the dog was quiet but alert, and hypothermic at 97.3ºF. The remainder of the physical examination was within normal limits. The dog was started on intravenous fluids supplemented with glucose. Rapid in-house assessment tests, venous blood gas analysis, complete blood count, and a full serum chemistry panel were performed. Fluids, supplemented with dextrose, were continued overnight and a constant rate infusion of hydrocortisone was started. A free catch urine and stool sample were also submitted for evaluation.
Review the laboratory data provided, and answer the following interpretive questions. (Abnormal and pertinent laboratory data have been included. Test results not included were within reference intervals.)
Questions:
- Given the dog’s clinical history and presentation, what is an unexpected finding in the hemogram results?
- What are the differential diagnoses for hypocholesterolemia and which is the most likely in this case?
- Presuming the dog’s azotemia resolves with fluid therapy, how would you explain the reduced concentrating ability of the kidney?