
Interpretation
Mesenchymal tumor – Synovial sarcoma (probable)
Explanation
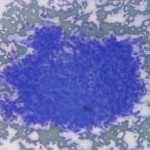
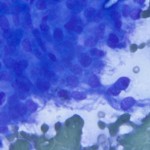
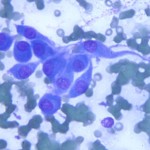
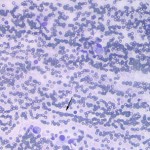
Differential diagnoses for an aggressive bony lesion (Question 1) include primary bone neoplasia, locally invasive soft tissue or metastatic neoplasia, and infection (bacterial or fungal).1 There was no evidence of inflammation in the aspirate, with only tissue cells being present, supporting a neoplastic process (Question 2). The tissue cells were spindled and found individually and in several dense aggregates, indicating a mesenchymal origin for the neoplasm (Question 3). Although the group of cells shown in Figure 1 may appear cohesive, Figure 2 shows that the cells have spindled, wispy cytoplasm with indistinct borders, consistent with a mesenchymal tumor. The tumor cells have round to slightly oval central to eccentric nuclei, single small nucleoli and display mild anisocytosis and anisokaryosis (Figure 3). They have a moderate amount of cytoplasm, which tapers away from each pole of the nucleus. Some individual cells were round, with eccentric nuclei and a vacuolated cytoplasm (resembling macrophages or synoviocytes in joint fluid aspirates) (Figure 4). In some areas, individualized cells appear to line up in rows (“windrowing”), which is seen in aspirates of viscous samples, such as joint fluid. The presence of viscosity suggested that the mass was involving the joint (or producing a viscous fluid such as synovial fluid or mucin), consistent with the described radiographic location of the mass crossing a joint. The main differential diagnoses for this case were a synovial sarcoma, histiocytic sarcoma and synovial myxoma.
|
|
|
|
|
Discussion
Synovial sarcoma (or synovial cell sarcoma) is an uncommon tumor in dogs, but is one of the most common joint tumor in dogs.1-7 It is a malignant neoplasm arising from primitive mesenchymal precursor cells outside the synovial membrane of joints and bursa.5 These precursor cells are theorized to then differentiate into either type A synoviocytes (phagocytic and resemble macrophages) or type B synoviocytes (fibroblastic).2,5,6 However, immunohistochemistry has shown three distinct populations of synoviocytes, including antigen-presenting dentritic cells.2 Middle aged, large breed dogs are most commonly affected, with a predisposition for flat-coated retrievers and golden retrievers,6 with no sex predilection.3,5,6 The most common presenting complaints are lameness and a visible or palpable mass associated with the affected joint.3,5 These clinical signs can be evident for months to even years prior to examination (as was the lameness in this case), which is attributable to the slow growing nature of synovial sarcomas.4,5 The most common sites are the large joints of extremities, particularly the stifle, elbow, and shoulder, although any joint and less commonly tendon sheaths can be affected.1,3-7 Synovial sarcomas are locally aggressive and the lameness can be attributed to the invasion of the neoplasm into the synovium, which is a tissue with a high number of pain fibers.3 They have a moderate to high metastatic potential (higher than typical soft tissue sarcomas), with the regional lymph nodes and lungs being the most common metastatic sites.6
Radiographic findings of the affected joint can range from radiographically normal to periarticular soft tissue swelling to ill-defined periosteal reaction to bony lysis involving bones on either side of the joint, depending on the stage of progression of disease.1 One retrospective study of 35 cases of synovial tumors in dogs found the three most common tumors were histiocytic sarcoma, synovial sarcoma, and synovial myxoma.2 Other reported joint tumors in dogs include fibrosarcoma, rhabdomyosarcoma, osteosarcoma, malignant fibrous histiocytoma, liposarcoma, hemangiosarcoma, malignant giant cell tumor of soft tissue, and undifferentiated sarcoma.2
There is a histologic classification scheme for synovial sarcomas that is routinely used in human medicine, which classifies tumors as monophasic or biphasic depending on the presence of one or both of the epithelial (synovioblastic) and mesenchymal (fibroblastic) cells within the tumor.2,3,5,6 Monophasic synovial sarcomas are typically composed of the mesenchymal component only.5 Due to the variability of the appearance of synovial sarcomas (depending on the proportions of these two components), the diagnosis of synovial sarcomas can be challenging on histopathology alone.3,5,6 Monophasic synovial sarcomas, for example, may be indistinguishable from fibrosarcomas and undifferentiated sarcomas.3,5 This is when tumor location, radiographic appearance, and biologic behavior can be useful in differentiating these tumors.5 This classification scheme is controversial in veterinary medicine and it is not consistently used.3,5,6 In addition, it has not been shown to have prognostic value in veterinary medicine with several studies showing no significant difference in survival time between dogs that had monophasic or biphasic tumors.3,5 Immunohistochemistry can aid in the diagnosis of synovial tumors. All synovial tumors are uniformly positive for vimentin.2 Synovial sarcomas are variably reactive for cytokeratin (epithelial marker).2,3,5 One study showed cytokeratin expression was associated with significantly shorter disease-free interval and survival time.5 Histiocytic sarcomas are more pleomorphic and express CD18.2,6 Malignant fibrous histiocytomas stain diffusely positive with smooth muscle actin.2 Synovial myxomas have a distinct pattern and can be diagnosed without immunohistochemical markers.2
A histologic grading scheme developed by Vail, et al. divides synovial sarcomas into grade I, II, or III based on degree of nuclear pleomorphism, number of mitotic figures per 10 high power (400x) fields, and proportion of the tumor that is necrotic.5 The histologic grade was shown to have prognostic value with the median survival time for grade III tumors being significantly worse (7 months) than grade I (48 months) or grade II (36 months) tumors.5
Limb amputation is the treatment of choice for synovial sarcomas due to the high rate of recurrence after local excision.1,4,5,6 Dogs treated with limb amputation have a median survival time of 850 days versus 455 days following marginal resection.3 Stump recurrence, following limb amputation, can occur and does so at a higher rate with synovial sarcomas than with other tumors for which amputation is recommended.6 Dogs with metastatic disease at the time of diagnosis have a median survival time of less than 6 months compared to 36 months or more if there is no evidence of metastasis.5 When metastatic disease is present at the time of diagnosis, palliative radiation can be done to provide pain relief and slow disease progression.1
Follow up
No evidence of metastatic disease was found on three-view thoracic radiographs. The patient underwent surgery for a right forelimb amputation without complication. The limb and adjacent lymph node (which was found to be mildly enlarged at surgery) were submitted for histopathologic examination. The dog was discharged on multiple different analgesic medications pending the biopsy results. The histopathologic diagnosis of the shoulder mass was a synovial cell sarcoma (see Figures 5 and 6 for representative images of the biopsy). The neoplasm was not graded. The tumor was completely excised and there was no evidence of metastasis in the submitted lymph node.
References
- Gibbons, DS et al. Palliative radiation therapy in the treatment of canine appendicular synovial sarcoma. J Am Anim Hosp Assoc. 2011; 47: 359-364.
- Craig, LE et al. The diagnosis and prognosis of synovial tumors in dogs: 35 cases. Vet Pathol. 2002; 39:66-73.
- Fox, DB et al. Canine synovial sarcoma: a retrospective assessment of described prognostic criteria in 16 cases (1994-1999). J Am Anim Hosp Assoc. 2002; 38:347-35.
- Hodge, SC. et al. What is your diagnosis? J Am Vet Med Assoc. 2007; 231:1203-1204.
- Vail, DM. et al. Evaluation of prognostic factors for dogs with synovial sarcoma: 36 cases (1986-1991). J Am Vet Med Assoc. 1994; 205:1300-1307.
- Withrow, SJ and DM Vail. Small animal clinical oncology. 4th ed. Saunders Elsevier. 2007.
- Yamate, Jyoji et al. Synovial sarcoma of the tendon and tendon sheath in a dog. J Vet Med Sci. 2006; 68:983-986.