
Aspirate from a liver in a dog
Case Information
A 12-year-old small spayed female mixed breed dog was presented as an emergency to the Cornell University Hospital for Animals (CUHA) with an acute onset of vomiting, lethargy and anorexia. The referring veterinarian had noted neutropenia, hypoglycemia and a mildly increased alkaline phosphatase activity on bloodwork along with a suspect hepatic abscess on point-of-care abdominal ultrasonographic examination. On examination by the emergency service at CUHA, the dog was dull and obtunded, 8-10% dehydrated, febrile (103.4°F), tachycardic (150 beats per minute), and had weak femoral pulses and cold extremities. A venous blood gas analysis revealed an acidemia (pH 7.29 units, reference interval [RI], 7.32-7.38 units) due to a primary metabolic alkalosis (bicarbonate concentration 18 mmol/L, RI, 20-25 mmol/L; base excess -9 mmol/L, RI, -4 to 0 mmol/L) with a compensatory respiratory alkalosis (pCO2 37 mmHg, RI, 38-46 mmHg). The strong ion difference ([sodium +potassium] – chloride) was within reference intervals at 40.3 mEq/L (36.7-46.5 mEq/L). Point-of-care testing showed hypoglycemia (35 mg/dL, reference interval) and hyperlactatemia (5.5 mmol/L, normal <2 mmol/L), but a normal packed cell volume, azostick (urea nitrogen concentration) and total solid concentration. The hyperlactatemia with the normal strong ion difference indicated a titration metabolic acidosis from hypovolemia and anaerobic metabolism. No other clinical pathologic testing was performed. A focused assessment sonography in trauma (FAST) abdominal scan showed a suspect hepatic abscess with no peritoneal fluid accumulation. The dog was treated with intravenous fluids, dextrose, anti-pain medication, and antibiotics for suspect sepsis.
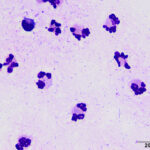
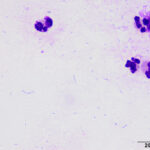
Several hours later, repeat abdominal ultrasonographic examination by the imaging section revealed a large (5 x 4 cm) cystic hepatic mass with an anechoic center and a thick hyperechoic vascularized rim. There was a concurrent diffuse moderate nodular hepatopathy, moderate diffuse peritonitis with a small amount of fluid accumulation (attributed to overnight fluid administration), a moderate diffuse enteropathy and mild right adrenomegaly. An ultrasonographic-guided aspirate of the cystic region of the liver was performed. Direct smears were stained with modified Wright stain. Examine the representative images and answer the questions below.
- Do the results support the clinical diagnosis of a hepatic abscess?
- Can you identify a cause for the cytologic findings?
|
|
|
Answers on next page