
Interpretation
Malignant melanoma with transudation and hemorrhage or diapedesis of erythrocytes (Question 3)
Explanation
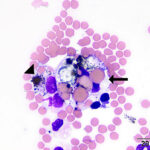
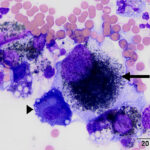
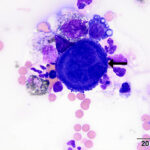
The cytospin preparation was of moderate to high cellularity. There were roughly equal proportions of non-degenerate neutrophils and macrophages with slighter fewer lymphocytes and rare mast cells. Macrophages were prominently erythrophagocytic (evidence of prior hemorrhage or RBC diapedesis) and many contained variable amounts of brown-black granules, consistent with melanin, in their cytoplasm (Figures 1-3, 3a). There was free melanin, likely from ruptured cells, in the background. There were also low numbers of round to spindled cells containing many small melanin granules (Figure 4, 4a). These cells had quite large round nuclei with smooth light chromatin and moderate amounts of light blue to colorless cytoplasm with distinct boundaries. Some of the cells were binucleated and the cells overall displayed moderate anisocytosis and anisokaryosis. They were interpreted to be melanocytes. There were also numerous reactive mesothelial cells (Figures 4-5, 4a-5a).
The low automated nucleated cell counts and mildly increased protein concentration classifies this as a transudative effusion (Question 1). Cytologically, the presence of melanocytes indicates the cause of the effusion is a neoplasm (i.e. melanoma), thus it could also be interpreted as a neoplastic effusion.
A Prussian blue stain could be used to rule out iron-containing pigments, such as hemosiderin (Question 2), although the pigment seen in these cells was not consistent with iron. We did perform this stain and the pigment was Prussian blue negative.
|
|
|
|
Discussion
Altogether, neoplastic effusions make up a minority of pleural and peritoneal fluids submitted for analysis in veterinary medicine. One report cited pyothorax and chylothorax as the most common causes of pleural effusions in dogs and cats, followed by neoplastic effusions, transudative effusions, and hemothorax.1 Exudative effusions constitute the majority of thoracic effusions in horses, with inflammatory effusions accounting for 53-91% of reported thoracic effusions.2-6 In contrast, neoplastic effusions overall account for somewhere between 5% and 38% of equine thoracic effusions,2,3,5 with lymphoma being the most commonly reported neoplasm.7,8 In contrast, melanoma is a rare cause of a body cavity effusion in horses. Although normal pleural fluid in horses (which is not typically aspirated) is expected to be a transudate, pathologic transudates in the thoracic cavity of horses are less common than exudates and are typically attributed to similar pathophysiologic processes as in other species (i.e. increased hydrodynamic forces from venous or lymphatic hypertension). In our case, the transudative effusion was likely secondary to the tumor obstructing or impeding with lymphatic drainage from the thorax.
Melanoma is a common, slow growing dermal neoplasm that is vastly overrepresented in older grey horses, accounting for 15% of all equine dermal neoplasms,9-11 and nearly all of those cases are grey horses.9,10,12 Melanomas have been infrequently reported in bay and chestnut horses.10 Arabian horses, in addition to some other breeds, have been reported as being overrepresented, however affected horses were also grey10,13,14 and it is unclear if there is a true breed disposition. Historically, dermal melanomas have been considered generally benign, however it is estimated that up to 80% of grey horses will develop a melanoma by 15 years of age.12,15,16 The most common sites of metastasis are regional lymph nodes and lungs, followed by the liver, spleen, blood vessels, and heart.17 Metastatic melanoma to the thoracic cavity is still rare and has been reported only a few times over the past several decades.8,17-21 There is only one case report, to our knowledge, in which melanophages and presumptive melanocytes were detected in both pleural or peritoneal fluid and peripheral blood in a horse with malignant melanoma.18 Primary intra-thoracic melanoma has not yet been confirmed in a horse. It is unknown what color the horse was in our case nor if there was any evidence of a dermal neoplasm, however statistically it is most likely that the horse was a grey Arabian stallion and had a primary dermal melanoma, possibly in the perineal region (a common location for this tumor).
Essentially all grey horses have inherited a gene colloquially known as the “grey gene”, which is a duplication in the 6th intron of the syntaxin-17 (STX17) gene.22 Both this gene and a neighboring gene, NR4A3, are over-expressed in grey horses as a consequence of this mutation. The end phenotypic result is a proliferation of melanocytes, although the exact mechanism by which these genes result in greying is still unknown and it has been hypothesized that the proliferation of melanocytes exhausts the stem cell supply in the region of the hair follicle resulting in depigmentation at a premature age.22,23 Perhaps unsurprisingly, horses with a homozygous genotype pf the mutated form of STX17 (STX17G) have a greater prevalence and severity of melanomas, in addition to more frequent color distortion, including vitiligo, than their heterozygous counterparts.24 Furthermore, the copy number of STX17G appears to increase as the behavior of the tumor becomes more aggressive.25 From an immunophenotypic perspective, Melan A, a popular immunohistochemical stain used to identify melanomas in humans and dogs,26 does not stain equine melanocytic tumors and other immunostains, such as that for the somatostatin receptor PNL2 are more reliable.27 However, PNL2 can also be positive in mature myeloid cells (such as neutrophils) in humans,26 and anecdotally appears to stain macrophages in veterinary patients, warranting that more work needs to be done to determine the clinical usefulness of this stain in our patients.
The presence of melanocytes with criteria of malignancy was essential for the diagnosis of malignant melanoma in this case. It is important to note that the mere presence of melanin-containing macrophages does not necessarily confirm the diagnosis of neoplasia. Membrane-associated melanosis is a commonly encountered phenomenon in many species, including pigs and ruminants. This is a benign accumulation of melanocytes in membrane surfaces including the pleura and leptomeningeal membranes and is not ascribed to have any pathologic significance in these species.28,29 However, melanosis has never been reported in the pleura of horses, although anecdotally it can occur in the leptomeninges of horses and neuromelanin-like pigments have been described in the pineal gland of horses.30 Therefore, macrophages containing melanin may, in theory, not be diagnostic alone for a malignant melanoma as a benign pleural melanosis could yield pleural melanophages, particularly in the presence of inflammation. In humans, pleural melanosis is considered an important differential diagnosis for the presence of melanin pigment on cytologic examination of pleural fluid,31 although the diagnosis of melanoma in pleural effusions is rare in humans as well.32,33 However, the presence of melanocytes, with cytologic criteria of malignancy, makes malignant melanoma the most likely explanation for the effusion in this case. In addition, neoplasia was suspected by the clinician, however no other information was provided in the history.
References
- Reetz JA, Suran JN, Zwingenberger AL, et al. Nodules and masses are associated with malignant pleural effusion in dogs and cats but many other intrathoracic CT features are poor predictors of the effusion type. Vet Radiol Ultrasound 2019;60:289-299.
- Smith BP. Pleuritis and pleural effusion in the horse: a study of 37 cases. J Am Vet Med Assoc 1977;170:208-211.
- Johns I, Marr C, Durham A, et al. Causes of pleural effusions in horses resident in the UK. Eq Vet Educ 2017;29:144-148.
- Sweeney CR. Causes of pleural effusion in the horse. Equine Vet Educ 1992;4:75-77.
- Wagner AE, Bennett DG. Analysis of Equine Thoracic Fluid. Vet Clin Pathol 1982;11:13-17.
- Chaffin MK. Thoracocentesis and pleural drainage in horses. Equine Vet Educ 1998;10:106-108.
- Mair TS, Brown PJ. Clinical and pathological features of thoracic neoplasia in the horse. Eq Vet J 1993;25:220-223.
- Sweeney CR, Gillette DM. Thoracic Neoplasia in Equids – 35 Cases (1967-1987). J Am Vet Med Assoc 1989;195:374-377.
- Cotchin E. Tumours of farm animals: A survey of tumours examined at the Royal Veterinary College, London, during 1950-60. Vet Rec 1960;72:816-822 & 823.
- Johnson PJ. Dermatologic Tumors (Excluding Sarcoids). Vet Clinics North Am Eq Pract 1998;14:625-658.
- Smith SH, Goldschmidt MH, McManus PM. A Comparative Review of Melanocytic Neoplasms. Vet Pathol 2002;39:651-678.
- Valentine BA. Equine Melanocytic Tumors: A Retrospective Study of 53 Horses (1988 to 1991). J Vet Intern Med 1995;9:291-297.
- Lerner AB, Cage GW. Melanomas in horses. Yale J Biol Med 1973;46:646-649.
- Seltenhammer MH, Simhofer H, Scherzer S, et al. Equine melanoma in a population of 296 grey Lipizzaner horses. Eq V J 2003;35:153-157.
- Gorham S, Robl M. Melanoma in the gray horse: The darker side of equine aging. Vet Med 1986;81:446-448.
- Mcfadyean J. Equine melanomatosis. J Comp Pathol Therap 1933;46:186-188.
- Metcalfe LV, O’Brien PJ, Papakonstantinou S, et al. Malignant melanoma in a grey horse: case presentation and review of equine melanoma treatment options. Irish Vet J 2013;66:22-22.
- Tarrant J, Stokol T, Bartol J, et al. Diagnosis of malignant melanoma in a horse from cytology of body cavity fluid and blood. Eq Vet J 2001;33:531-535.
- Milne JC. Malignant melanomas causing Horner’s syndrome in a horse. Equine Vet J 1986;18:74-75.
- Murray MJ, Cavey DM, Feldman BF, et al. Signs of Sympathetic Denervation Associated With a Thoracic Melanoma in a Horse. J Vet Intern Med 1997;11:199-203.
- Recknagel S, Nicke M, Schusser GF. Diagnostic assessment of peritoneal fluid cytology in horses with abdominal neoplasia. Tieraerztl Prax Ausg G Nutztiere 2012;40:85-93.
- Rosengren Pielberg G, Golovko A, Sundstrom E, et al. A cis-acting regulatory mutation causes premature hair graying and susceptibility to melanoma in the horse. Nat Genet 2008;40:1004-1009.
- MacKay RJ. Treatment Options for Melanoma of Gray Horses. Vet Clin North Am Equine Pract 2019;35:311-325.
- Curik I, Druml T, Seltenhammer M, et al. Complex Inheritance of Melanoma and Pigmentation of Coat and Skin in Grey Horses. Plos Genetics 2013;9:9.
- Sundström E, Imsland F, Mikko S, et al. Copy number expansion of the STX17 duplication in melanoma tissue from Grey horses. BMC Genomics 2012;13:365.
- Ramos-Vara JA, Miller MA. Immunohistochemical Identification of Canine Melanocytic Neoplasms With Antibodies to Melanocytic Antigen PNL2 and Tyrosinase: Comparison With Melan A. Vet Pathol 2010;48:443-450.
- Ramos-Vara JA, Frank CB, DuSold D, et al. Immunohistochemical expression of melanocytic antigen PNL2, Melan A, S100, and PGP 9.5 in equine melanocytic neoplasms. Vet Pathol 2014;51:161-166.
- Wohlsein P, Deschl U, Baumgartner W. Nonlesions, unusual cell types, and postmortem artifacts in the central nervous system of domestic animals. Vet Pathol 2013;50:122-143.
- Mellau LS, Nonga HE, Karimuribo ED. A slaughterhouse survey of lung lesions in slaughtered stocks at Arusha, Tanzania. Prev Vet Med 2010;97:77-82.
- Cozzi B. Cell types in the pineal gland of the horse: an ultrastructural and immunocytochemical study. Anat Rec 1986;216:165-174.
- Murali R, Loughman NT, McKenzie PR, et al. Cytological features of melanoma in exfoliative fluid specimens. J Clin Pathol 2009;62:638-643.
- Chhabra A, Mukherjee V, Chowdhary M, et al. Black Pleural Effusion: A Unique Presentation of Metastatic Melanoma. Case reports in oncology 2015;8:222-225.
- Wang Q, Chen J, Dassarath M, et al. Primary malignant melanoma of the pleura with rapid progression: A case report and literature review. Oncol Lett 2015;9:2713-2715.
Authored by: C. Shiprack (intern) and edited by T Stokol