
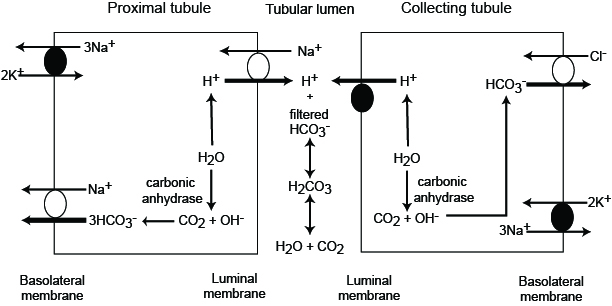
Filtered bicarbonate is “reclaimed” in proximal and collecting tubules by hydrogen excretion (linked to sodium absorption in the proximal tubules and direct hydrogen excretion in the collecting tubule).
a) In the proximal convoluted tubule (PCT) cell, carbonic anhydrase generates bicarbonate and hydrogen from water and carbon dioxide. Sodium in filtered urine is resorbed in exchange (with a sodium/hydrogen cotransporter) for the hydrogen produced from carbonic anhydrase. The excreted hydrogen then combines with filtered bicarbonate. This forms the weak acid, carbonic acid, which then disassociates to produce water and carbon dioxide in the urine (tubular lumen). The bicarbonate created by carbonic anhydrase is transported, with the resorbed sodium, into the blood via a basolateral (blood side) sodium/bicarbonate cotransporter. Thus, through carbonic anhydrase and sodium absorption, the proximal tubules “reclaim” the filtered bicarbonate (or, in reality, generate new bicarbonate which replaces that lost in the urine, so there is no net gain of bicarbonate). The energy for the Na/H transporter is driven by the Na/K exchanger on the basolateral side of the renal tubular membrane. This creates a negative potential within the renal tubule (an exception to the electroneutrality law) since 2 potassium enter the cell for 3 sodium which leave the cell and enter blood. This negative potential drives the movement of the basolateral sodium/bicarbonate exchanger (and more bicarbonate leaves the cell than sodium with transporter). Angiotensin II stimulates activities of both the basolateral sodium/bicarbonate cotransporter and the luminal sodium/hydrogen antiporter (thus promoting sodium and bicarbonate retention).
b) In the collecting tubules, carbonic anhydrase again does its work and generates bicarbonate and hydrogen. The filtered bicarbonate is “reclaimed” by the active excretion of hydrogen by a hydrogen ATPase-pump (not in exchange for sodium). The bicarbonate generated by carbonic anhydrase is excreted back into blood in exchange for chloride, via a chloride/bicarbonate exchanger (the energy for this exchanger is derived from the sodium/potassium pump located on the basolateral membrane. A similar hydrogen ATPase does operate in the PCT, but the Na/H exchanger described above is responsible for about 2/3 of the “reclaimed” bicarbonate. Aldosterone directly activates the hydrogen ATPase pump and stimulates the basolateral chloride/bicarbonate exchanger, thus promoting hydrogen excretion and bicarbonate retention.
With both methods of bicarbonate generation (sodium dependent in the PCT and hydrogen dependent in the DCT), the resorbed bicarbonate is actually not the original molecule filtered into the urine. However, there is no net gain of bicarbonate with this system (in effect, the filtered bicarbonate is being reclaimed, albeit indirectly). In this way, the kidney excretes hydrogen and generates bicarbonate simultaneously.