
MCH
The mean cell hemoglobin or MCH is a calculated red blood cell (RBC) index that gives an indication of the average amount (in pg) of hemoglobin in the red blood cells (RBC). It is calculated from the spectrophotometrically measured hemoglobin concentration (after lysis of RBCs) and RBC count so it represents the amount of hemoglobin per RBC. It is thus affected by hemoglobin content and volume (e.g. a smaller RBC will have less hemoglobin by virtue of size alone because you cannot make more hemoglobin than normal).
The formula used to calculate MCH is:
MCH (pg) = Hemoglobin concentration (g/dL) ÷ RBC count (mill/µL)
Because the MCH is dependent on the cell volume (e.g. it will be increased if the cells are larger than normal, tracking with the MCV, even if they are contain less hemoglobin), we usually refer to the MCV (macrocytic, normocytic, microcytic) and MCHC (hypochromic, normochromic, hyperchromic) to characterize red blood cell size and hemoglobin content per unit volume (or concentration), when describing an anemia, and do not include the MCH in this assessment. To expand on this concept, animals with a high MCV from a regenerative anemia with numerous larger than normal immature RBC (e.g. polychromatophils) will have a high MCH. This is because the MCH increases as the cell volume or size increases, even though immature RBCs, such as polychromatophilic RBCs, have less hemoglobin per unit volume than a mature RBC. However, the MCHC will be decreased in polychromatophils (maybe not below the lower reference limit) because this takes into account the volume changes (MCHC = Hb ÷ [HCT] or Hb ÷ [MCV x RBC]) and shows hemoglobin concentration per unit volume. Conversely, the MCV and MCH will track low in animals with smaller RBCs. The low MCH could be due to cells that have lower volume/smaller size than normal and a normal hemoglobin content (MCHC would be normal) or cells that of normal volume but have a lower hemoglobin content (MCHC would be low) or both.
There are instances where the MCH does not track with the MCV. For example, with in vitro RBC swelling with storage, the MCV increases but the uptake of water dilutes the hemoglobin, leading to a decrease in MCH and MCHC, despite the increase in MCV. The reverse occurs with shrinkage of RBCs, e.g. hyponatremia or excess EDTA, where the MCV decreases but MCH and MCHC increases. In addition, the MCH will track with the MCHC and not the MCV when the spectrophotometrically measured hemoglobin is disproportionately increased compared to the RBC (denominator in MCH) or HCT (denominator in MCHC), e.g. false increases in the measured hemoglobin concentration with lipemia or when there is in vitro hemolysis or in vivo intravascular hemolysis (where RBCs and HCT are decreased in relation to the hemoglobin concentration). With hemolysis of any cause, the lysed RBCs will not be counted or contribute to the HCT but the spectrophotometrically measured hemoglobin concentration is unchanged as it does not matter if it is “free” or inside the cells when we measure it as the machine lyses the RBCs to measure the hemoglobin by its light absorption properties (around 540 nm).
CH

The MCH is a calculated value based on the measured hemoglobin concentration, after lysing the cells and measuring the free hemoglobin based on its absorption with a spectrophotometer, and RBC count. In contrast, the CH or mean cellular hemoglobin content (in pg) is obtained from optical (light scatter) measurement of the hemoglobin content (amount) within each intact red blood cell, which is averaged from all intact red blood cells, as shown in the image to the right. The CH can be considered as the “optical equivalent” of the MCH but only provides information from intact red blood cells. Since CH is the amount of hemoglobin within cells, it is similarly affected by changes in RBC volume, like the MCH.
Why are we telling you about this? As indicated above, the optically measured hemoglobin concentration and related indices, CH and CHCM, are more accurate than the spectrophotometrically measured hemoglobin and related indices, MCH and MCHC, when there is a false increase in the latter hemoglobin concentration, e.g. moderate to severe lipemia. The CH and CHCM are also more accurate than the MCH and MCHC with in vitro or in vivo intravascular hemolysis, because the spectrophotometrically measured hemoglobin is disproportionately higher than the RBC count or hematocrit, both of which only measure intact and not lysed RBCs. We provide these optically measured results on our hemograms under the circumstances mentioned above, i.e. when we think the MCH and MCHC (and hemoglobin) are falsely increased for some reason.
Note that the CH and CHCM are affected similarly to the MCH and MCHC with RBC swelling with storage or hyperosmolality (MCH, MCHC, CH and CHCM decrease, while MCV increases) and cell shrinkage with EDTA or hyponatremia (MCH, MCHC, CH and CHCM increase while MCV decreases).
HC
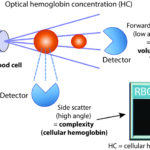
The ADVIA also provides another optically measured hemoglobin measurement, called the optical hemoglobin concentration or HC. This HC is a calculated result based on dividing the laser-based side scatter (measure of cellular hemoglobin concentration) by forward scatter (measure of the RBC volume), however this result is usually not provided with hemograms nor looked at frequently.