
Cerebrospinal fluid from a cat
Case information
A 5.5-year-old female spayed, domestic longhair cat presented to the neurologic service for hindlimb paralysis. Three days before presentation, the cat was lethargic and had difficulty jumping onto counters. The cat also vocalized when attempting to jump, which was interpreted as pain. The referring veterinarian performed bloodwork, which was normal, and made the presumptive diagnosis of a saddle thrombus. The neurologic signs progressed to hindlimb paraplegia the day before presentation and the cat appeared to be painful. The neurologic signs remained static over 24 hours until referral and the cat was eating, drinking, urinating and defecating normally.
On examination, the cat was bright, alert and responsive. A neurologic examination did not demonstrate any defects in the cranial nerves and propioception was normal in the front legs. There was decreased proprioception in the hindlimbs and pain on palpation of the thoracolumbar spine. Withdrawal reflexes were normal in all four limbs and patellar reflexes were normal in the hindlimbs. The defect was localized to T3-L3. Magnetic resonance imaging showed contrast enhancement in several sections of the thoracolumbar spinal cord. A hemogram, chemistry profile and lumbosacral cerebrospinal fluid (CSF) tap (0.3 mL) were submitted to the clinical pathology laboratory. No abnormalities were detected on the hemogram. A mildly decreased ALT activity (25 U/L, reference interval 35-176 U/L), decreased serum iron concentration (51 ug/dL, reference interval 53-145 U/L) and mildly increased creatine kinase (CK) activity (682 U/L, reference interval 73-388 U/L) were the only abnormal findings on the chemistry profile. The CSF had a total nucleated cell count of 1448 cells/uL, red blood cell count of 488 cells/uL and a total protein of 3275 mg/dL.
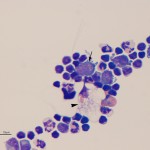
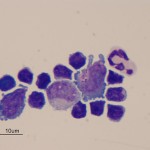
Evaluate the representative photomicrographs of the CSF tap and answer the questions posed below:
- What type of pleocytosis is present in the cat’s CSF?
- What is the identity and diagnostic relevance of the cell labeled with the arrow in Figure 1?
- What is the identity and diagnostic relevance of the cell labeled with the arrowhead in Figure 1?
- What additional tests are indicated?
|
|
|
Answer on next page